
47 Years Later: A Case of an Unrepaired Tetralogy of Fallot
Written by: Dr. Andrew Shanes
Edited by: Dr. Joann Hsu
Case Presentation
47 year old male with a past medical history of “heart problem,” prior stroke with left sided residual weakness, presenting to the ED for right knee pain s/p trip and fall 6 days ago. States tripped and fell forward, struck his head and his right knee, and since has been having increased pain and swelling. No LOC. No Chest pain, SOB, lightheadedness or other associated symptoms.
Initial Vitals: BP 144/90, HR: 92, RR: 20, Temp: 36.8, SpO2: 80%
Physical Exam:
SKIN: Warm, dry. (+) perioral cyanosis, (-) rash
HEAD: (+) small area of ecchymosis to the right forehead. Otherwise; (-) scalp swelling, (-) tenderness.
CHEST AND RESPIRATORY: (-) rales, (-) rhonchi, (-) wheezes; breath sounds equal bilaterally.
HEART AND CARDIOVASCULAR: Regular rate and rhythm, (+) holosystolic murmur (-) gallop.
ABDOMEN AND GI: Soft; (-) tenderness, (-) guarding, (-) rebound, (-) Murphy's, (-) McBurney's
LOWER EXTREMITIES: (+) edema and tenderness to medial aspect of right knee, extending proximally. (-) edema to the remainder of RLE. Full ROM. (+) bilateral UE finger clubbing. Otherwise; (-) deformity, (-) other tenderness, (+) equal pulses in upper and lower extremities
NEURO AND PSYCH: Cranial nerves grossly intact; Strength grossly intact. Sensation grossly intact.
Additional History: Upon further questioning, the patient notes that he has had a “heart condition” since he was born, cannot recall the name of it, but as a teenager moved to the United States from China and has seen cardiologists but ultimately decided to never have surgery. Patient states that his oxygen level is “always low” and he has no increased difficulty breathing compared to his baseline.
Decision was made to perform limited beside echocardiogram:
Initial POCUS shows abnormality in the ventricular septal wall (PSL 1 above), and upon putting color doppler, imaging was highly suspicious for a VSD.
The patient's aortic outflow tract also appeared to be enlarged and received flow from both the LV and RV, concerning for an “overriding aorta” (PSL 2 above).
Additional views were obtained showing RV strain (likely chronic) in the PSS (below) as well as significantly enlarged RA and RV chambers, as noted in the A4C view (below).
Remainder of ED Course: Patient underwent additional imaging including a CTA Chest that showed atrophic main and central pulmonary arteries and extensive mediastinal and upper abdominal collateral vessels. Patient was ultimately admitted to the CCU where he had an official echocardiogram that showed similar and additional findings, all consistent with a diagnosis of unrepaired Tetralogy of Fallot.
What is Tetralogy of Fallot?
Tetralogy of Fallot (TOF) encompasses a spectrum of cardiac defects that stem from anterocephalad deviation of the ventricular outlet septum during cardiac development in utero.
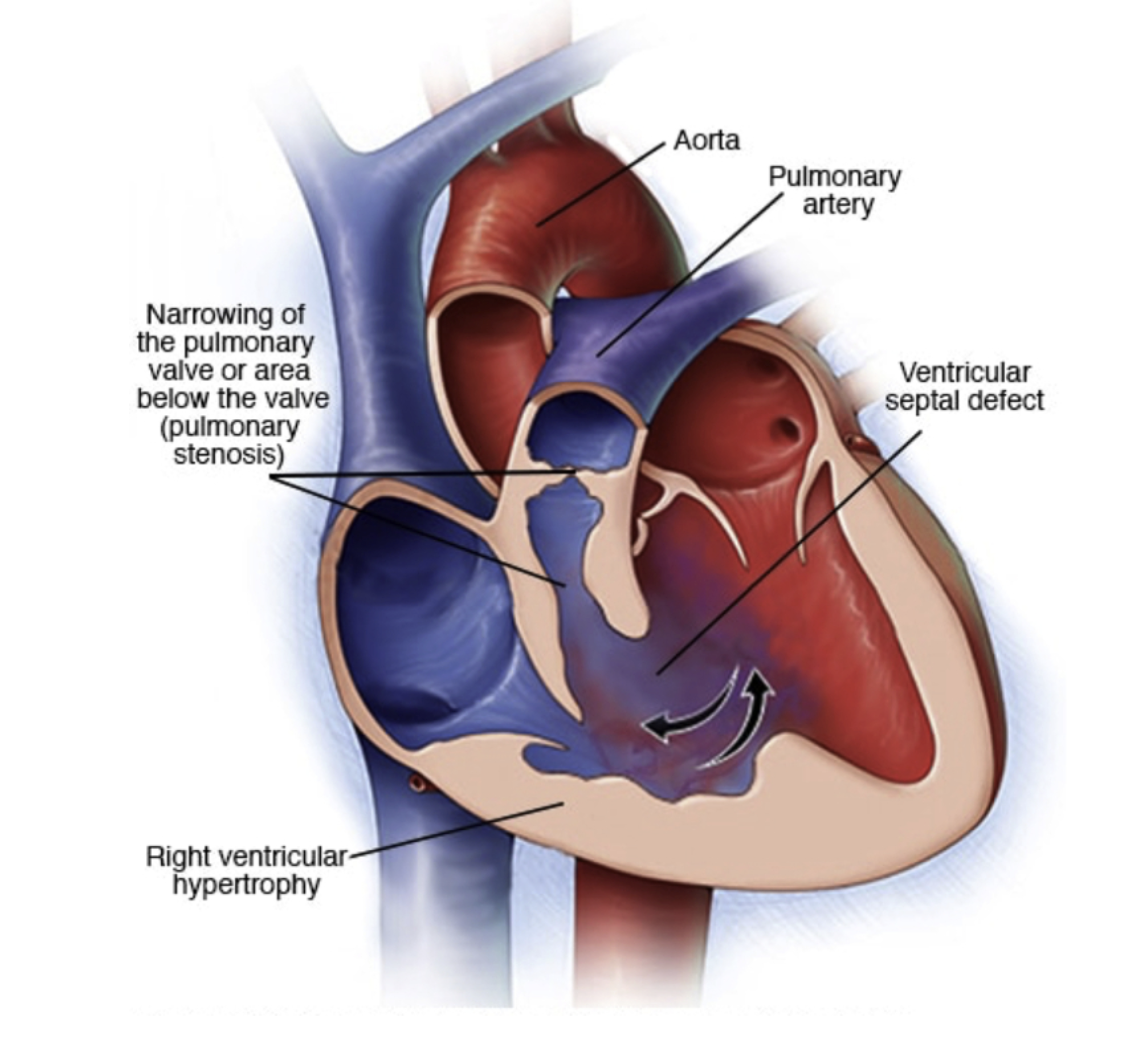
Four Components:
Ventricular septal defect (VSD)
Overriding Aorta
Pulmonary stenosis
Right ventricular (RV) infundibular narrowing and RV hypertrophy
History and Epidemiology
Tetralogy of Fallot is a cyanotic congenital cardiac defect that was first described by Steno of Denmark in 1672 and later named for Fallot of Marseilles, who in 1888 described it as a single pathological process.
Tetralogy of Fallot accounts for 5%-10% of all congenital heart defects and is seen in 1 out of every 3000 live births.
Since the time of first discovery 400 years ago, and it’s first surgical repair in 1944 by Blalock, Taussig, and Thomas, treatment strategies have come a significantly long way. Today, complete repair of TOF is performed before six months of age with low mortality (<2%) and long-term survival rates are excellent (85%-90%).
However, life expectancy for unrepaired TOF is still very low.
< 50% survive past 3 years of age
< 25% survive past 10 years
Only 1-2% survive past the age of 40 years
Pathophysiology
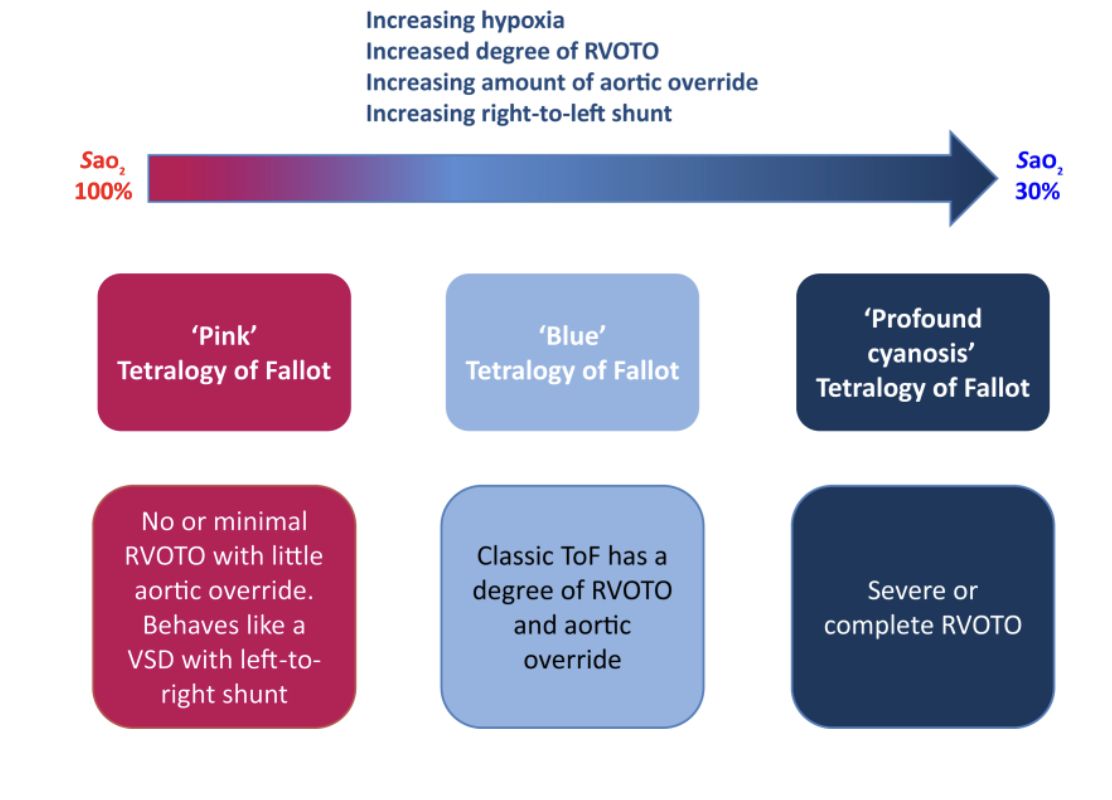
Tetralogy severity is predominately based on degree of RVOT obstruction and pulmonary stenosis and depending on the degree of obstruction/stenosis, patients with TOF can be pink or cyanotic at baseline.
“Pink” TOF babies have adequate pulmonary blood flow and can be monitored clinically and by serial echo until repair
“Cyanotic” TOF has ductal dependent pulmonary blood flow and requires PGE administration following birth to keep the PDA open and ensure sufficient pulmonary blood flow until intervention or repair is performed.
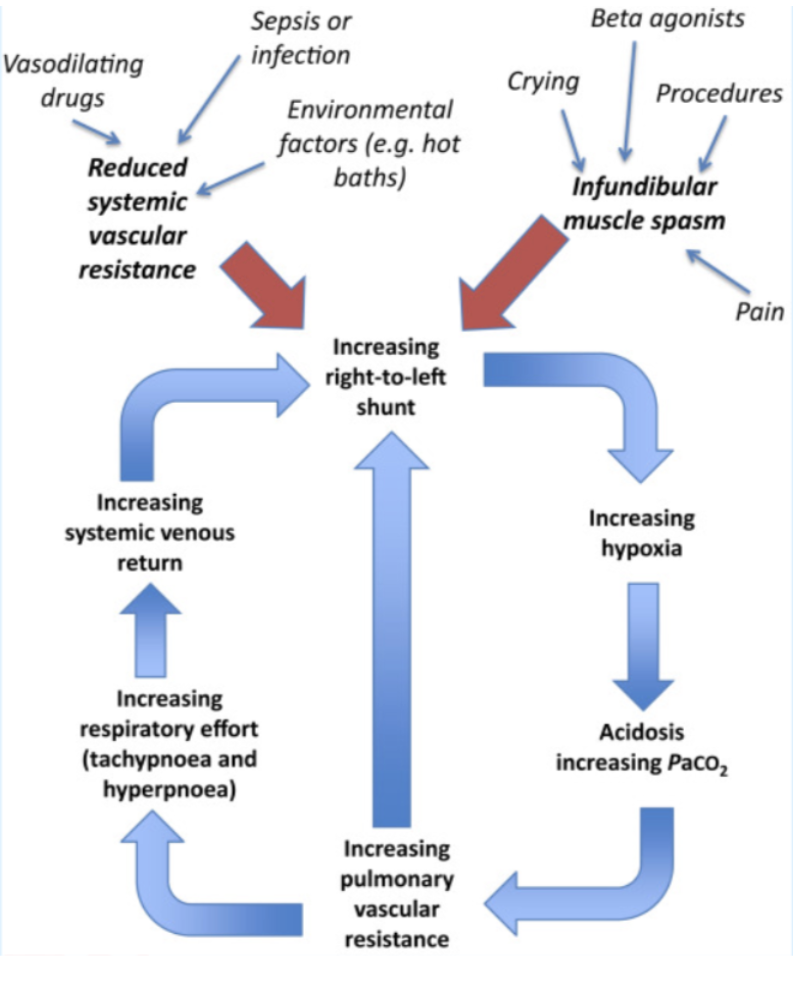
“Tet Spells”
Certain events (fever, stress, crying, etc.) can cause either a decrease in Systemic Vascular Resistance (SVR), an increase in Pulmonary Vascular Resistance (PVR) PVR, or both.
This decreases pulmonary blood flow and leads to increased pressure in the RV, creating a new pressure gradient, resulting in a reversal of flow and shunting of blood, right-to-left across the VSD.
This results in even more deoxygenated blood traveling through the overriding aorta to the periphery and decreased oxygen delivery to tissues, presenting as cyanosis.
The decrease in oxygenation triggers a reflex increase in respiratory effort (hyperpnea) as well as increased acidosis, further exacerbating right-to-left shunting, creating this self-perpetuating cycle.
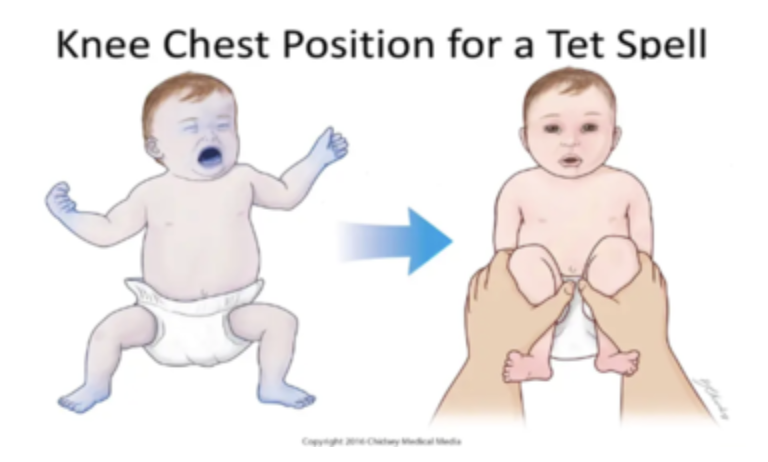
The “knee to chest” position in infants, or squatting in older children, can help reverse “Tet Spells.” This position compresses the leg veins and femoral arteries, increasing venous return to the heart and increasing systemic vascular resistance (SVR). This helps raise pressure in the left ventricle, helping reverse the right-to-left shunt and forcing more deoxygenated blood through the pulmonary valve for oxygenation rather than across the VSD and into the aorta.
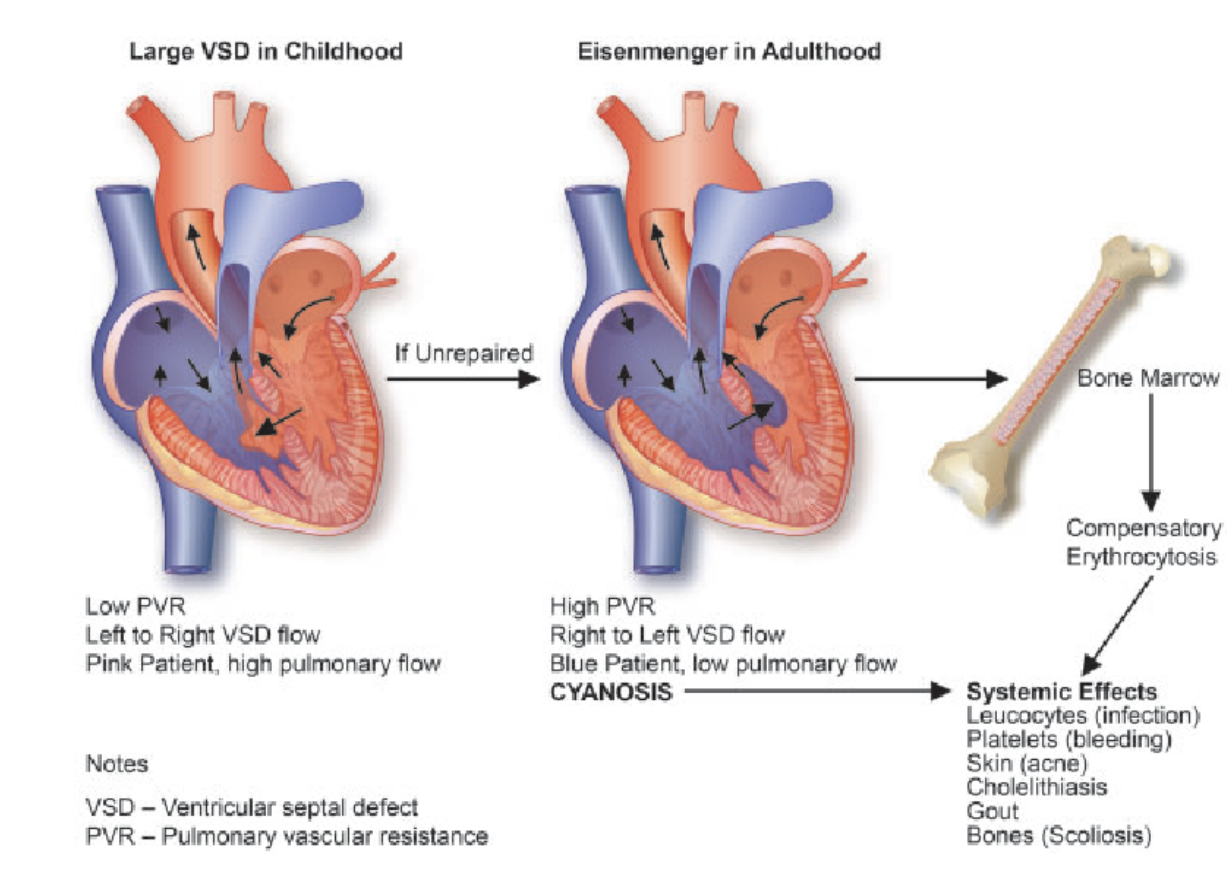
Chronically Unrepaired ToF
In Patients who never undergo repair, over time, increased PVR causes increased RV pressures, resulting in RV hypertrophy. This creates persistent right-to-left shunting across the VSD, known as Eisenmenger Syndrome.
Over time, this will result in:
Low pulmonary flow (pulmonary arteries can become atrophic/stenosed)
Chronic cyanosis and hypoxia
High EPO → compensatory erythrocytosis (secondary polycythemia)
These chronic changes overall increases risk for:
Infection
Hyperviscosity (stroke, CKD)
Right Sided Heart Failure
Cholelithiasis (increased RBC turnover → hyperbilirubinemia)
Gout
Scoliosis
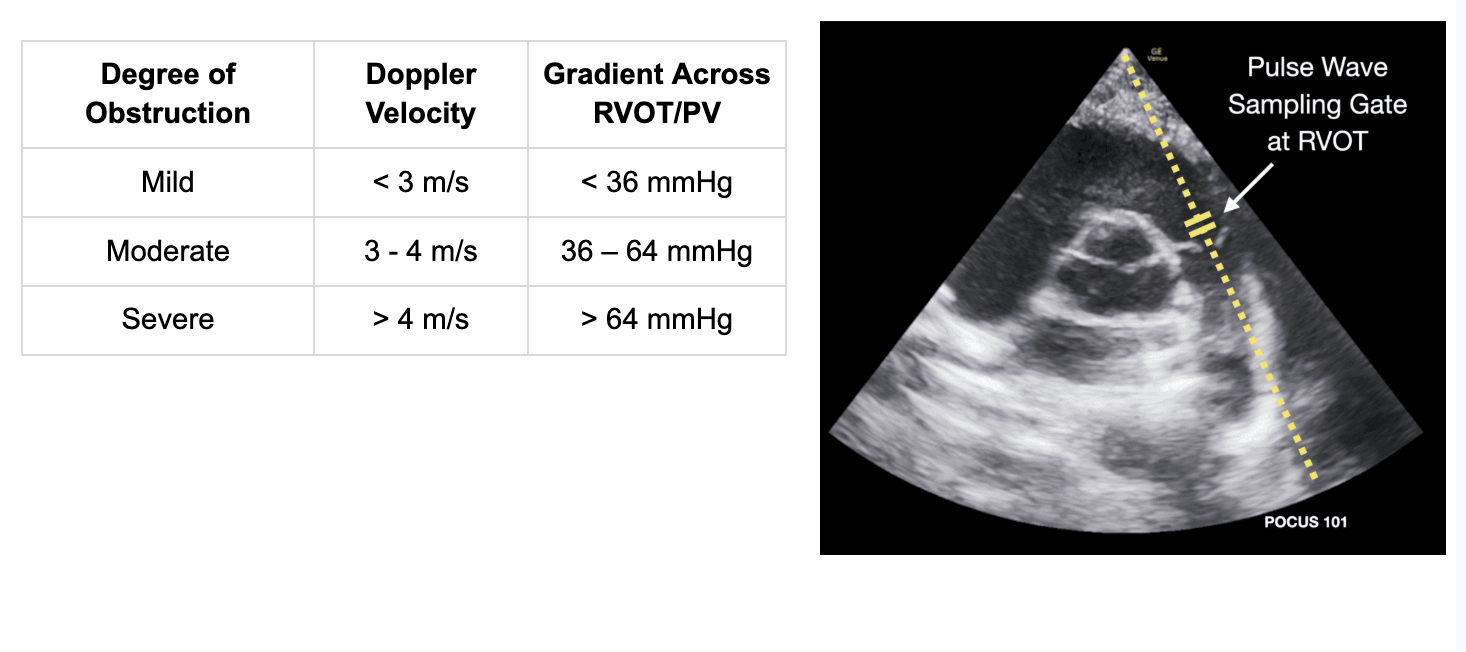
Utilizing Ultrasound in Tetralogy of Fallot
Hyper-cyanotic spells are caused by RVOT obstruction during ventricular contraction, which causes R → L shunting at the VSD and decreased pulmonic blood flow.
Pulse Wave Doppler can help measure the RVOT velocity and VTI (Velocity Time Integral)
Continuous Wave Doppler can help determine type of RVOT obstruction:
Dynamic (A): late-peaking “lobster claw” or dagger-shaped Doppler signal
Fixed/Supravalvar (B): mid-systolic peak, more symmetric Doppler signal
Obstruction in series (C): overlapping Doppler patterns
Obstruction in Series is most common in TOF as there is dynamic narrowing below the pulmonary valve with fixed stenosis along the pulmonary valve or main pulmonary artery.
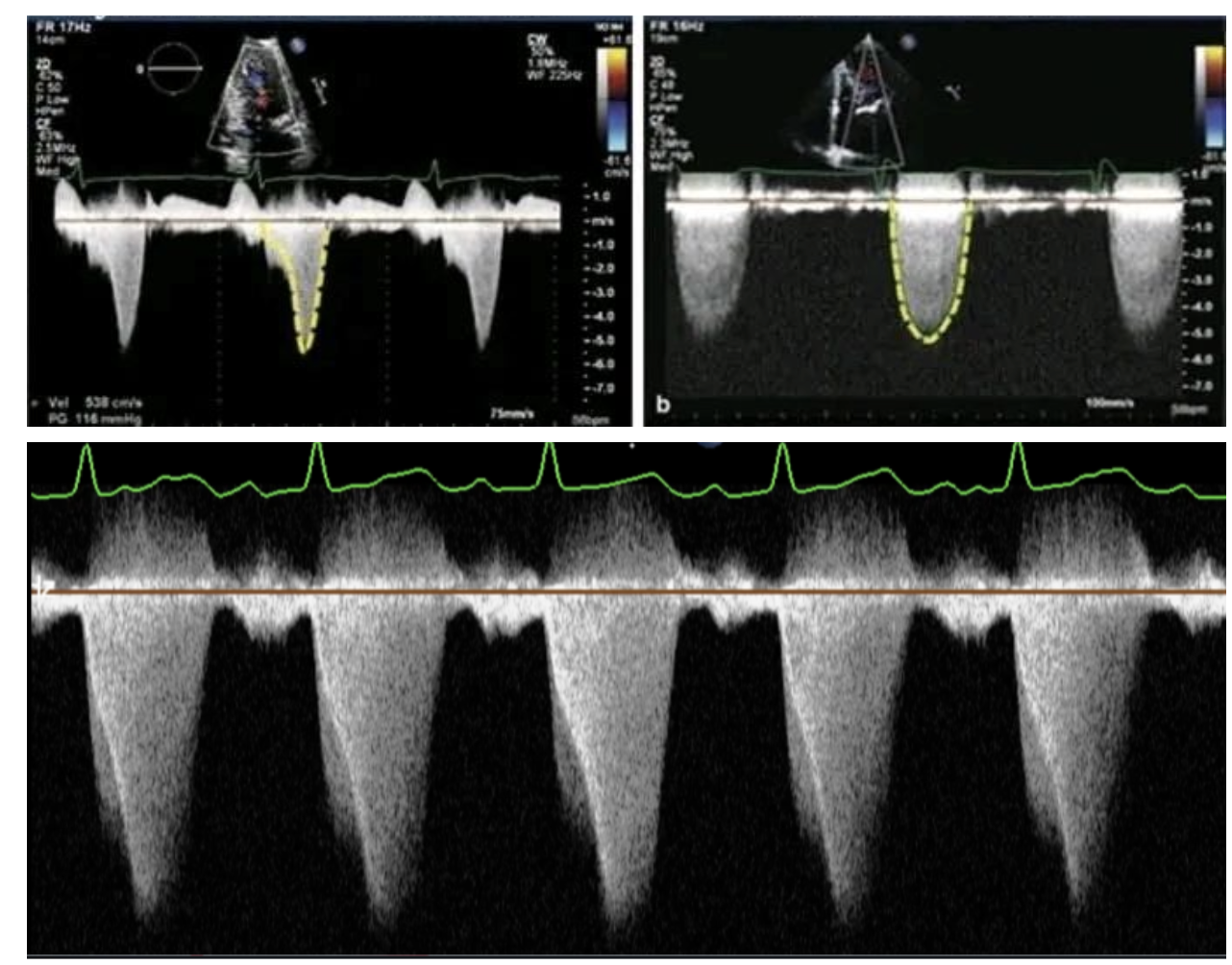
A (Top Left): Dynamic Obstruction
B (Top Right): Fixed Obstruction
C (Bottom): Obstruction in Series
Overall, ultrasound can be used to:
Identify VSD size and location
Identify pulmonary artery size and valve stenosis
Identify degree of fixed and dynamic RVOT obstruction
Identify patients at higher risk for hypercyanotic spells
Guide surgical planning
Happy scanning!
Resources:
EM:RAP. Corpendium. Tetralogy of Fallot. https://www.emrap.org/corependium/chapter/recc9rciQBNMP2AcT/Tetralogy-of-Fallot
Pedecho. Tetralogy of Fallot. https://pedecho.org/library/chd/tetralogy-fallot
POCUS 101. Right ventricular ultrasound: Qualitative and quantitative assessments. https://www.pocus101.com/right-ventricular-ultrasound-qualitative-and-quantitative-assessments
StatPearls Publishing. (2024). Tetralogy of Fallot. In StatPearls. https://pmc.ncbi.nlm.nih.gov/articles/PMC9586846/
WikiEM. Tetralogy of Fallot. https://wikem.org/wiki/Tetralogy_of_Fallot
Wilson, R., Ross, O., & Griksaitis, M. J. (2019). Tetralogy of Fallot. BJA Education, 19(11), 362–369. https://doi.org/10.1016/j.bjae.2019.07.003
YouTube. Tetralogy of Fallot [Video]. https://www.youtube.com/watch?v=FC7IRCtyMIo