
Large Bowel Obstructions
Written by: Dr. Richard Gallardo
Edited by: Dr. Joann Hsu
Case Presentation
84 year old male with PMH of HTN, HLD, DM, and sigmoid volvulus s/p detorsion and open sigmoidectomy w/ end to side anastomosis on 10/29/25 presented for evaluation of abdominal pain x 4 days a/w multiple episodes of NBNB vomiting and 1 daily episode of non-bloody, watery diarrhea each morning. Also endorsed the sensation of intense gurgling sounds whenever he ate.
Diagnosis… LARGE bowel obstruction!!
Patients with large bowel obstructions may present with abdominal pain, abdominal distension, and failure to pass any stool/flatus.
Can also have nausea/vomiting and dehydration.
When considering underlying causes of large bowel obstructions, some of the more common causes are underlying colorectal cancer, inflammatory bowel disease, food blockage, volvulus, and strictures.
Important things to look out for in your HPI and PE when considering large bowel obstruction in your differential are abdominal distension, minimal or absent flatus, changes in bowel habits including diarrhea for partial obstructions, weight loss, and rectal bleeding.
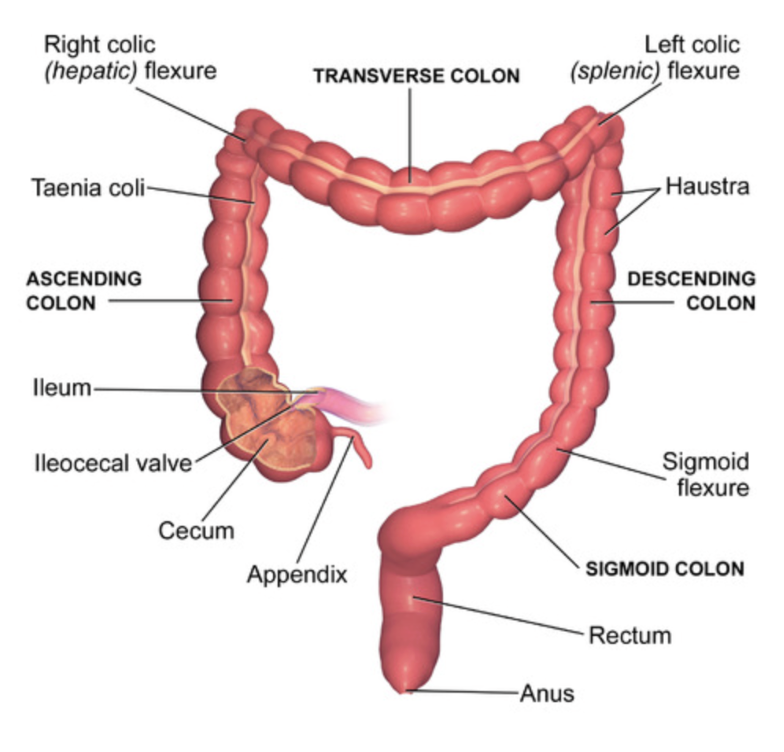
LARGE bowel obstructions can occur at any site, however, most commonly occurs at the sigmoid colon.
LBO: Ultrasound Findings
Diameter/Thickness
LBO on ultrasound will show a diameter of > 4.5 cm and thickness > 3 mm. The bowel wall is typically ≤ 3mm and ≤ 2 mm when distended
Haustra
Haustra are spaced and far apart. This differs from the plicae circulares of the small bowel.
A Lines
A-lines are reverberation artifacts seen on Ultrasound when beams interact with air. If seen inside the bowel, indicative of air-fluid levels inside bowels.
Abnormal peristalsis
“To and fro” movement of peristalsis indicative of obstruction. Normal peristalsis will have unidirectional flow
!!!Ultrasound has also been specifically evaluated for the diagnosis of LBO with a sensitivity of approximately 85% in one study!!
Comparison to SBO
The small bowel has plicae circulares as opposed to the haustra of the large bowel. Plicae circulares are circumferential and are seen much closer together.
When evaluating for SBO on ultrasound, may see Keyboard sign due to accentuation of the bowel wall due to edema. The diameter needed to identify SBO on ultrasound is >2.5 cm.
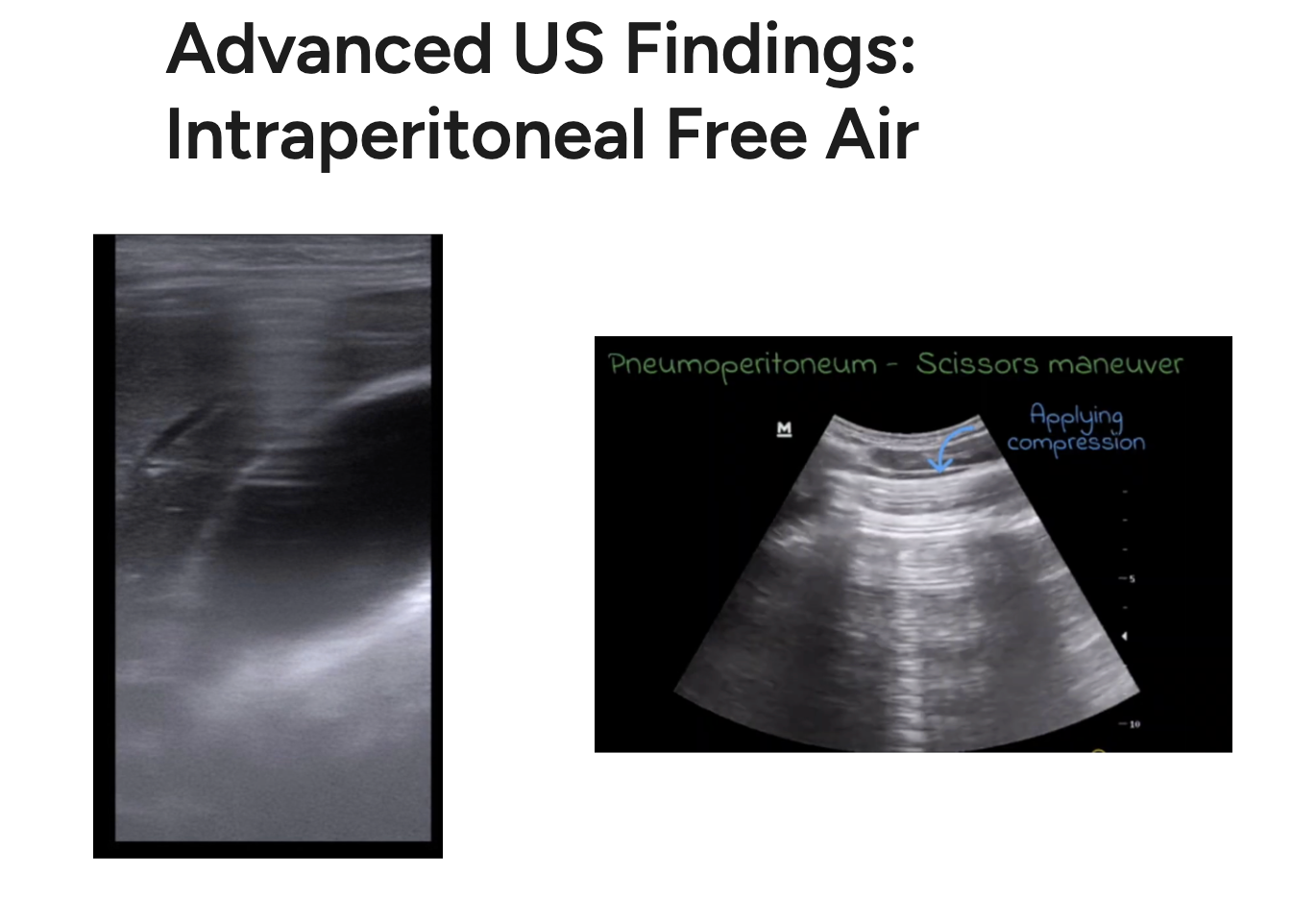
Enhanced Peritoneal Strip Sign (EPSS)
The interface between bowel and air creates a “stripe”. This finding has a sensitivity of 100% and a specificity of 99%.
Scissor maneuver: Slight pressure is applied to displace free air. Subsequently release of pressure will cause the free air to return into view. This has a sensitivity of 94% and a specific of 100%.
Happy Scanning!
References
Li RT, Zhao Y, Zou XJ, Shu HQ, Zhou T, Pan SW, Gao XH, Huang HY, Liu H, Shang Y. Overview of point-of-care ultrasound in diagnosing intestinal obstruction. World J Emerg Med. 2022;13(2):135-140. doi: 10.5847/wjem.j.1920-8642.2022.048. PMID: 35237368; PMCID: PMC8861339.
Lieske B, Marietta M, Meseeha M. Large Bowel Obstruction. [Updated 2024 Nov 9]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK441888/
Nelms DW, Kann BR. Imaging Modalities for Evaluation of Intestinal Obstruction. Clin Colon Rectal Surg. 2021 Jul;34(4):205-218. doi: 10.1055/s-0041-1729737. Epub 2021 Jun 2. PMID: 34305469; PMCID: PMC8292005.
https://my.clevelandclinic.org/health/diseases/bowel-obstruction
Asrani A. Sonographic diagnosis of pneumoperitoneum using the 'enhancement of the peritoneal stripe sign.' A prospective study. Emerg Radiol. 2007 Apr;14(1):29-39. doi: 10.1007/s10140-007-0583-3. Epub 2007 Mar 9. PMID: 17347768.
https://onlinelibrary.wiley.com/doi/10.1002/jcu.20055
https://nephropocus.com/2020/09/25/a-lines-all-over-the-abdomen/