
A Split Decision: Identifying Aortic Dissection with Ultrasound
Written by: Dr. Andres Somoza
Edited by: Dr. Joann Hsu
You hear a medical resuscitation activation called overhead.
A 55-year-old man is rushed into triage from the hospital’s main entrance. Staff report he was agitated, hypotensive, and unable to provide a clear history.
He repeatedly complains of severe right upper extremity pain.
On initial exam:
Mental status: Alert but confused, oriented only to self
Right arm: Cold with no palpable pulses
Vitals: Hypotensive with clinical concern for rapid deterioration
Something is clearly wrong. The asymmetric limb findings and hypotension raise concern for some sort of vascular catastrophe.
Fortunately, we can perform POCUS.
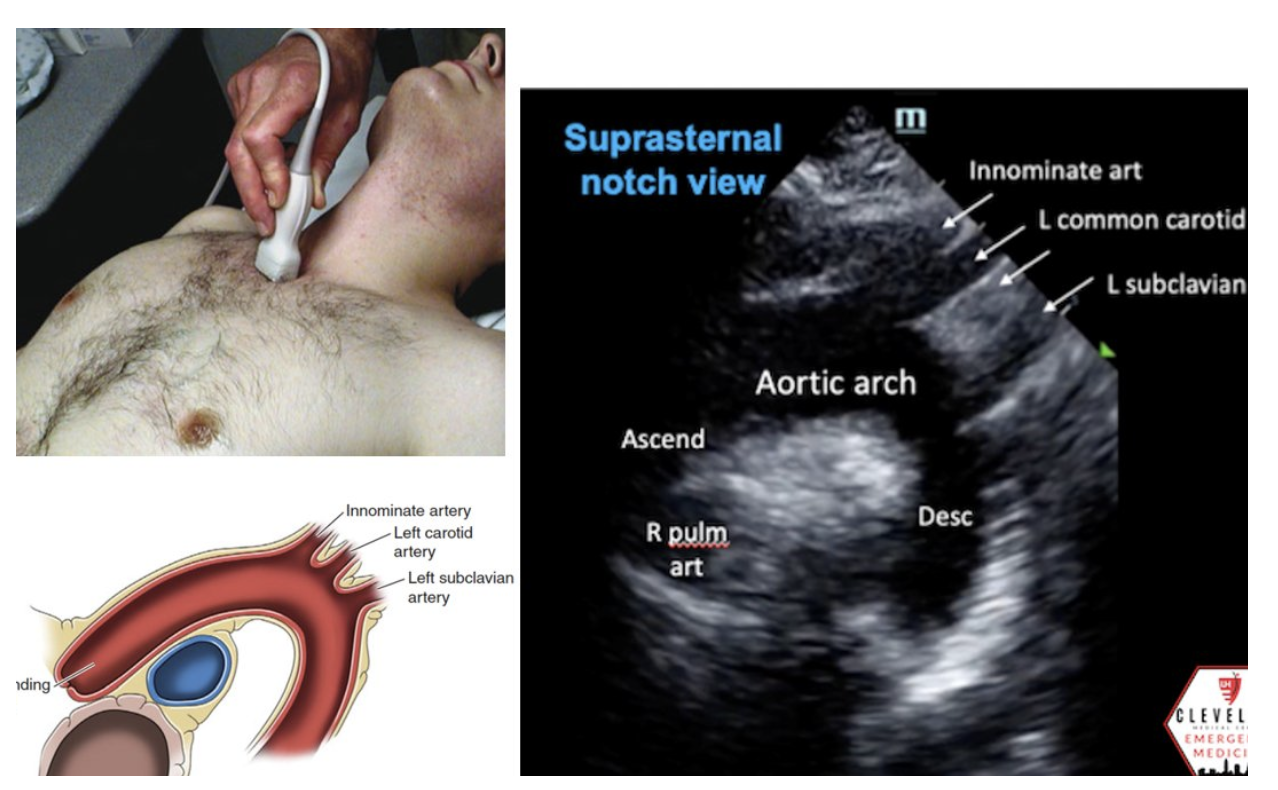
How to Obtain the Suprasternal Notch View
While the parasternal long view is helpful in identifying aneurysmal dilation of the aortic root and can even potentially show aortic dissection, the suprasternal notch view is an essential view when clinical suspicion is high for dissection. The suprasternal notch view provides a long-axis view of the thoracic aorta, including the ascending aorta, the arch, its three main branches, and the descending aorta. It is especially useful when evaluating for thoracic aortic aneurysm or aortic dissection.
Technique
Use a phased array probe in cardiac mode.
Position the patient supine, with the neck gently extended as tolerated.
Place the probe in the suprasternal notch.
Point the indicator toward the patient’s head, then rock the tail superiorly and rotate slightly clockwise toward the patient’s left shoulder to align with the thoracic aortic arch.
What you should see
Ascending aorta
Aortic arch
Descending thoracic aorta
Often the three major arch branches:
Brachiocephalic trunk
Left common carotid
Left subclavian artery
Doppler pearl
If obtained, color Doppler can help orient the view: in the suprasternal notch window, red flow toward the probe in the ascending aorta and blue flow away from the probe in the descending aorta.
Image 1 & 2: Parasternal long axis
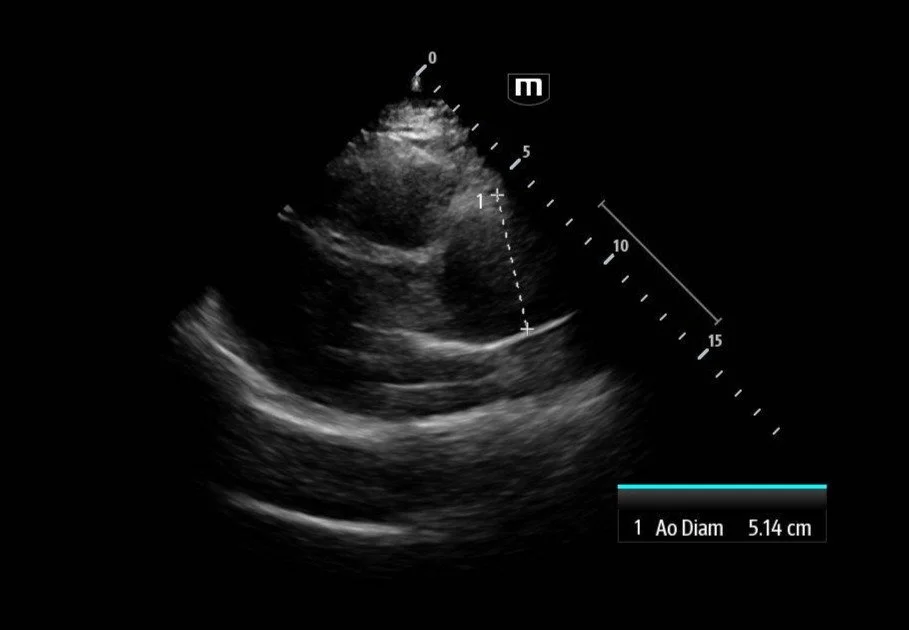
Interpretation: Parasternal long-axis view demonstrating marked dilation of the aortic root, measuring approximately 5.1 cm, concerning for proximal aortic pathology. Preserved EF and no effusions noted.
Teaching point:
Normal aortic root diameter: < 3.7–4.0 cm
A diameter >4 cm should raise concern for aneurysm or dissection
Image 3 - 5: Suprasternal notch
Interpretation: Dilated aortic arch including both ascending and descending aorta with linear echogenic structure within the lumen consistent with an intimal flap, as well as appearance of true and false lumens within the arch.
Ultrasound Findings in Aortic Dissection
Intimal flap within the lumen
Double lumen appearance
Ascending aortic dilation
Aortic arch involvement on suprasternal view
Possible aortic regurgitation in proximal dissections
Dissections may be seen in the ascending aorta, aortic arch, or descending abdominal aorta, and that ascending dissections can also cause aortic regurgitation and a diastolic murmur.
Classification
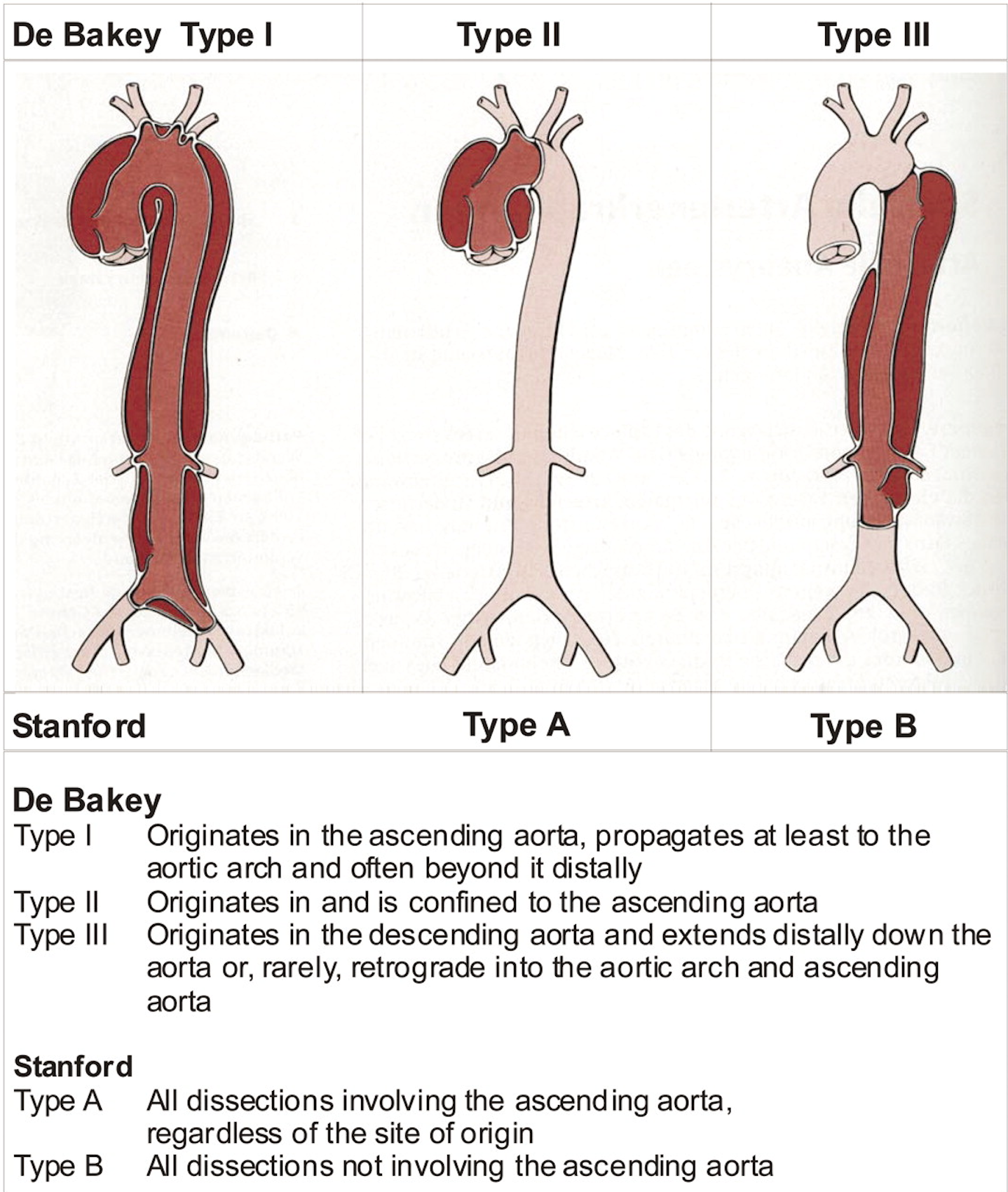
Typical Management of Aortic Dissection
For suspected aortic dissection, bedside priorities are:
Recognize it early
Control shear stress
Obtain definitive imaging
Get surgical consultation immediately for Type A disease
In general, Type A dissection is a surgical emergency, while Type B dissection is often managed medically unless complicated. If bedside TTE is negative but suspicion remains high, clinicians should proceed to CTA or TEE if feasible.
ED Course
Laboratory results revealed:
Lactate 5
Creatinine 1.8
CTA demonstrated Type A aortic dissection with:
Origin at the aortic root
Extension through the thoracic aorta
Involvement of:
Right brachiocephalic artery
Right subclavian artery
Left subclavian artery
The right axillary artery was not opacified, explaining the patient’s right arm pain and lack of a radial pulse in that arm.
Initial management included:
IV fluids
Analgesia (morphine)
Vasopressors for worsening hypotension
Central venous access
Blood transfusion
Immediate thoracic surgery consultation
After diagnosis:
IV antihypertensive therapy (labetalol) to reduce shear stress.
Definitive Treatment
The patient underwent emergent surgical repair with the Bentall procedure which includes replacement of the aortic root, ascending aorta, and aortic valve.
Outcome:
No complications
Patient recovered and was discharged home.
Key Teaching Points
1. Consider aortic dissection in patients with:
Pulse deficits
Limb ischemia
Hypotension
Altered mental status
2. POCUS findings that raise suspicion
Dilated aortic root
Intimal flap
Aortic arch dilation
3. The suprasternal notch view
Directly visualizes the aortic arch
Can reveal dissections missed on standard cardiac views
4. Management priorities
Reduce shear stress (beta-blockade)
Confirm diagnosis with CTA
Immediate surgical consultation
Happy scanning!
References:
Dinh V. Aorta ultrasound made easy: step-by-step guide. POCUS 101. Accessed March 5, 2026.
Isselbacher EM, et al. Aortic Dissection: New Frontiers in Diagnosis and Management. Circulation. 2003;108(5):628-635. doi:10.1161/01.CIR.0000087009.16755.E4.
Malekan R, Spielvogel D, Lansman SL. The completion Bentall procedure. Ann Thorac Surg. 2011;92(3):e73-e74. doi:10.1016/j.athoracsur.2011.03.083.
Reim P, Moore L, Minalyan A, Dinh V. RUSH exam ultrasound protocol: step-by-step guide. POCUS 101. Accessed March 5, 2026.