
The Ball’s In Your Court: A Case of Testicular Rupture
Written by: Dr. Hannah Weisman
Edited by: Dr. Joann Hsu
Case Presentation:
34 year old male with no PMHx who presents to the ED for evaluation of right testicular pain after a large object flew into his groin while working. Patient states he fell to the ground 2/2 pain. He denies head strike or LOC. Reports pain in right testicle, worse than the left testicle. Reports swelling in the R testicle as well. Endorses dysuria but denies hematuria. No nausea, vomiting.
Physical Exam: GU: (+) swollen right testicle, high rising compared to left, circumcised, (+) small abrasions to left and right inner thigh, no active bleeding. Cremasteric reflex intact BL.
What can we do next to aid in diagnosis? Ultrasound!!
A Stepwise Approach to Testicular Ultrasound:
Select the linear probe on the testicular or ocular setting - this will provide less thermal energy to the testicles which are sensitive to heat
Scan through both testicles with the buddy view (owl’s eye), compare both sides. You can compare normal to abnormal using this view on quick glance
Scan the normal testicle first
Scan in transverse and longitudinal
Assess the epididymis. Pro-tip: if the epididymis is hyperemic (more blood flow than normal) or enlarged (>1x1 cm) you should consider the diagnosis of epididymitis.
Scan the other testicle
Perform doppler testing to confirm blood flow to both testicles
Be sure to assess for both venous and arterial blood flow
Pro tip: in testicular torsion, venous flow is usually the first to go (before arterial flow) before there is no flow at all
This is what we see:
Right Testicle is shown above.
Notice how the echotexture of the testicle is not homogenous all the way through, which should catch your eye as a potential abnormal finding.
It is important to also note that the anechoic area to the R of the screen can be hematocele, abscess (less likely), varicocele, or hydrocele. Clinical context is very important to making the correct diagnosis with ultrasound.
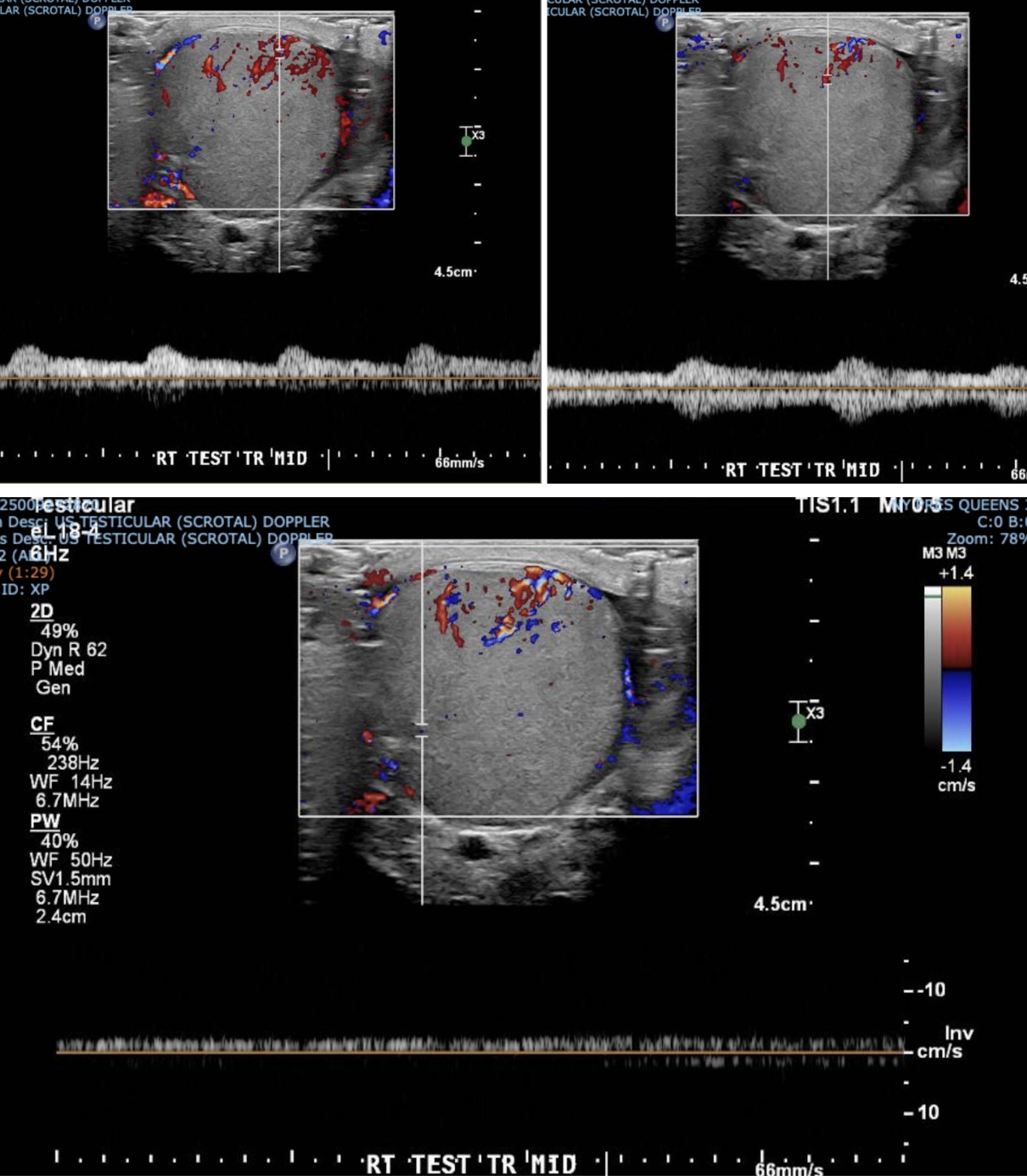
We made sure to confirm blood flow to BL testicles. Just because a patient has testicular rupture does not mean they do not have testicular torsion as well!
What is Testicular Rupture?
It is clinically defined as the disruption of the tunica albuginea, the fibrous covering of the testis. This disruption results in the extrusion of testicular content into the scrotal sac.
Etiology:
Blunt Trauma
This is the most common cause of rupture. It typically results from sports injuries, motor vehicle accidents, or direct blows to the groin.
Penetrating Injuries
Less common but often more severe. Examples include gunshot wounds, stab wounds, or animal bites requiring immediate exploration.
Compression
Rupture occurs when the testicle is compressed against the pubic bone with a force exceeding 50 kg, causing the tunica to tear.
Main Ultrasound Findings:
The main sign of testicular rupture on ultrasound is irregular testicular contour, extrusion of testicular contents, or heterogeneity of the testicular tissue.
Other findings can include a hematocele. A hematocele is a collection of blood within the tunica vaginalis. While not diagnostic of rupture alone, a large hematocele is highly suspicious for underlying testicular injury.
I want to reiterate that color doppler is imperative for determining vascular integrity, which will ultimately assist in providing the correct disposition for the patient.
For a Patient with Testicular Injury:
Absent Flow: Indicates ischemia or infarction, requiring immediate surgical salvage.
Decreased Flow: Compare with the contralateral healthy testis. Asymmetric flow suggests injury.
Hyperemia: Occasionally seen in surrounding tissues due to inflammation.
Management:
Consult urology as soon as possible. Depending on the viability of the testicular tissue the patient may need to go for surgery to remove the nonviable testicular tissue, or if it is a more severe injury, they will need complete orchiectomy of the injured testicle. If the injury is not very severe and the testicle is determined to be stable, the patient can be observed with close outpatient follow up.
Back to Our Patient:
Our patient had a very mild case of testicular rupture. Urology decided to admit the patient for serial testicular exams and repeat testicular ultrasound to demonstrate stability of the patient's injury. The patient was ultimately discharged with close urology follow up.
Takeaways:
Ultrasound is essential for diagnosis - It is the primary imaging tool. Look for tunica discontinuity and heterogeneous parenchyma.
Time is Tissue - Prompt diagnosis guides emergent surgical exploration. Early salvage rates are high.
Be suspicious - as a provider you should have high suspicion for testicular rupture in blunt trauma with associated large hematoceles or severe pain.
Happy scanning!
References:
1. Urotrauma Guideline 2020: AUA Guideline. Morey AF, Broghammer JA, Hollowell CMP, McKibben MJ, Souter L. The Journal of Urology. 2021;205(1):30-35. doi:10.1097/JU.0000000000001408.
2. Use of Ultrasonography for the Diagnosis of Testicular Injuries in Blunt Scrotal Trauma. Buckley JC, McAninch JW. The Journal of Urology. 2006;175(1):175-8. doi:10.1016/S0022-5347(05)00048-0.
3. Best Practices Guidelines Management of Gentiunrinary Injuries. Niels Johnsen, Hunter Wessells, Krystal Archer-Arroyo, et al. American College of Surgeons (2025)
4. Rational Approach to Diagnosis and Management of Blunt Scrotal Trauma. Chandra RV, Dowling RJ, Ulubasoglu M, Haxhimolla H, Costello AJ. Urology. 2007;70(2):230-4. doi:10.1016/j.urology.2007.03.064.
5. Tunica Vaginalis Graft Use for Repair of Traumatic Testicular Rupture: A Case Report. Masih S, Damodaran S, DaJusta DG. Urology. 2023;179:164-165. doi:10.1016/j.urology.2023.05.029.
6. Management of Testicular Rupture After Blunt Trauma in Children. Pogorelić Z, Jurić I, Biočić M, et al.
Pediatric Surgery International. 2011;27(8):885-9. doi:10.1007/s00383-011-2873-9.
7. A Conservative Approach to Testicular Rupture in Adolescent Boys. Cubillos J, Reda EF, Gitlin J, Zelkovic P, Palmer LS. The Journal of Urology. 2010;184(4 Suppl):1733-8. doi:10.1016/j.juro.2010.03.114.