
HOCUS POCUS
Written by: Dr. Sabrina Lee
Edited by: Dr. Joann Hsu
Just another day in the pediatric ED:
17 year old male with no past medical history comes in after a witnessed syncopal episode today while doing basketball warm-ups at school. He felt lightheaded and dizzy prior to passing out. He denies chest pain or shortness of breath. The syncopal episode lasted for about 1 minute. There was no shaking activity. Family history includes dad with a history of “weak heart muscles” but no other history of sudden cardiac death.
Initial Vitals:
HR 89
BP 157/72
RR 18
SpO2 98%
Temp 37 C
What would be your initial differentials for this patient?
More common reasons for syncope in a pediatric patient may include:
Vasovagal syncope
Orthostatic hypotension
Seizure
Can’t-miss differentials to think about include:
EKG abnormalities - think QT BRIDE findings!
Hypertrophic Obstructive Cardiomyopathy (HOCM)
Hypoglycemia
(This is a very abbreviated list but it can be much more expansive depending on clinical presentation and history!)
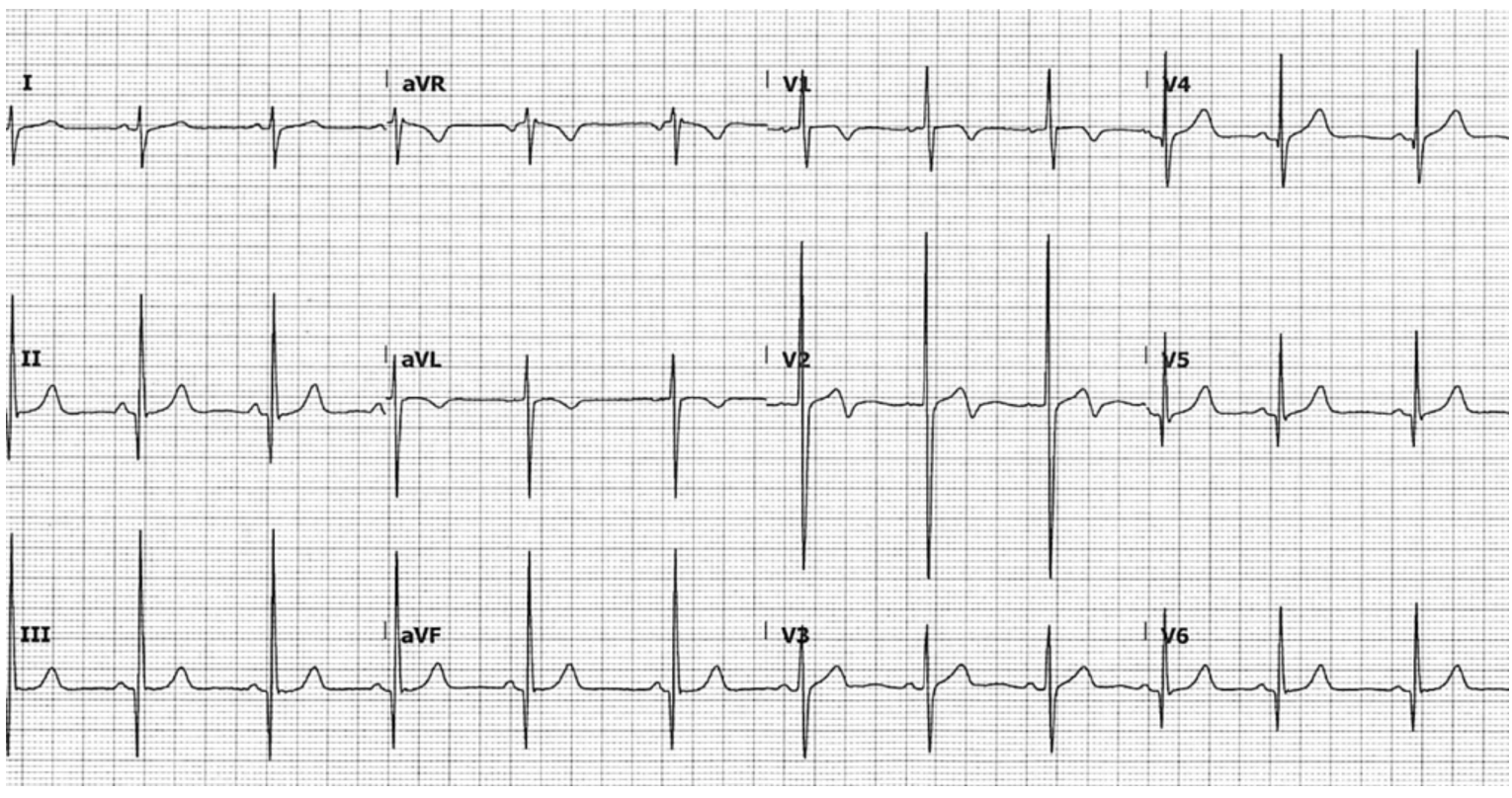
EKG was performed on arrival…

What do you see?
ST depressions and T wave inversions in the inferior leads
ST elevations in the anteroseptal leads
High voltage Q waves in the anteroseptal leads
Looks like Seamen’s Sign, which is QRS complexes touching or overlapping in 2 contiguous precordial leads
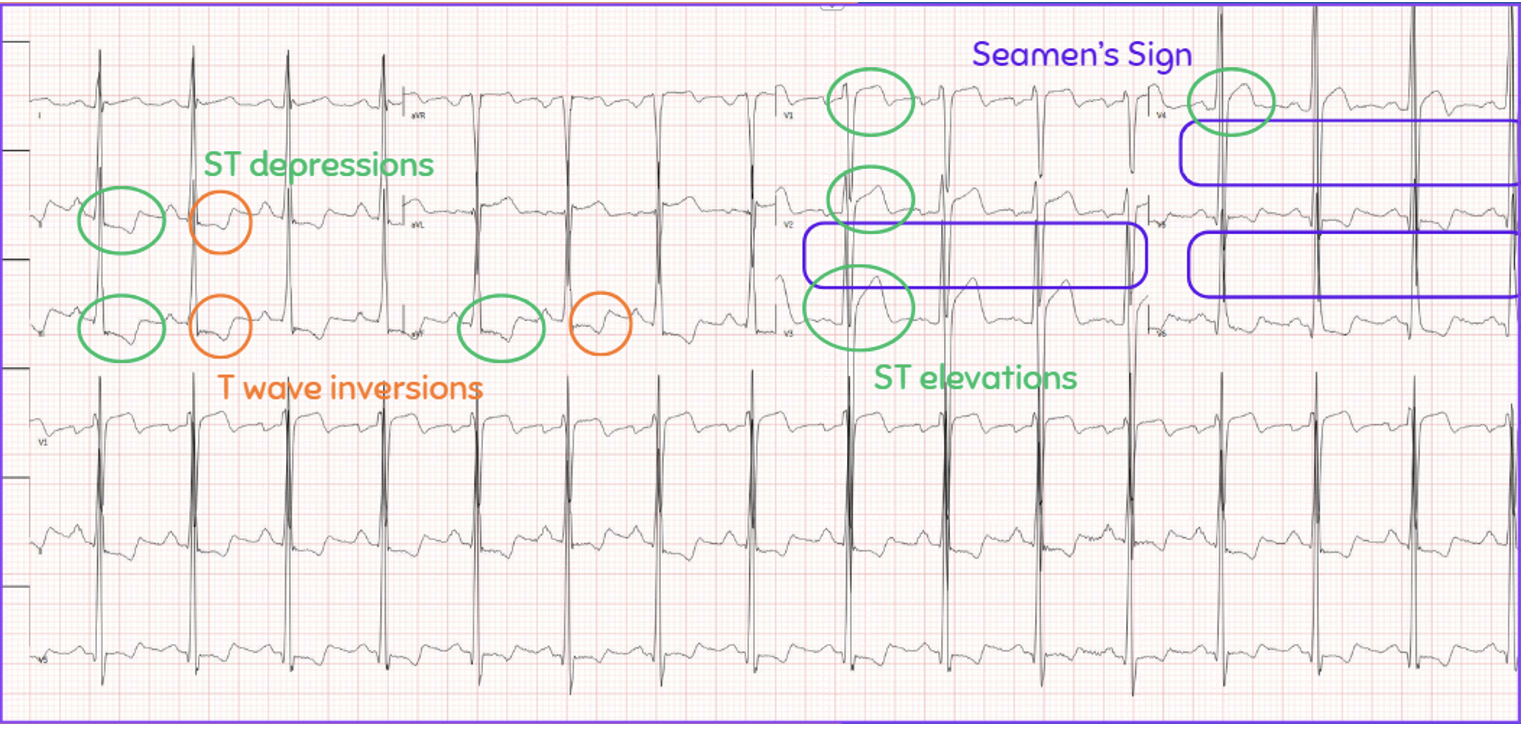
These EKG findings are concerning for left ventricular hypertrophy (LVH) or hypertrophic cardiomyopathy (HCM).
If only there was a way to evaluate for HCM at bedside…well, there is! Using our handy dandy point-of-care ultrasound!
Hypertrophic Cardiomyopathy (HCM)
Genetic mutation of the sarcomeres leading to hypertrophy of cardiac walls
Can progress into diastolic heart failure and reduced left ventricular function
Commonly has a harsh midsystolic crescendo-decrescendo murmur
Can be obstructive or non-obstructive
Hypertrophic Obstructive Cardiomyopathy (HOCM) makes up about 70% of HCM
Affects ~1 in 500 people
10% of patients are diagnosed
6% of patients are symptomatic → this leads to a delay in diagnosis!
#1 cause of sudden cardiac death in young people!
Symptoms
Most patients will be asymptomatic
Those who do develop symptoms will have:
Exertional syncope
This is the most concerning symptom as it may indicate left ventricular outflow tract obstruction with possible ventricular arrhythmias
Chest pain
Dizziness
Dyspnea on exertion
Palpitations
Symptoms will be exacerbation with exertion
EKG Findings
According to Life in the Fast Lane, HCM will show:
Left ventricular hypertrophy
High voltage in precordial leads
Nonspecific T wave and ST segment abnormalities
“Needle/dagger-like” Q waves in lateral and inferior leads
Left atrial enlargement
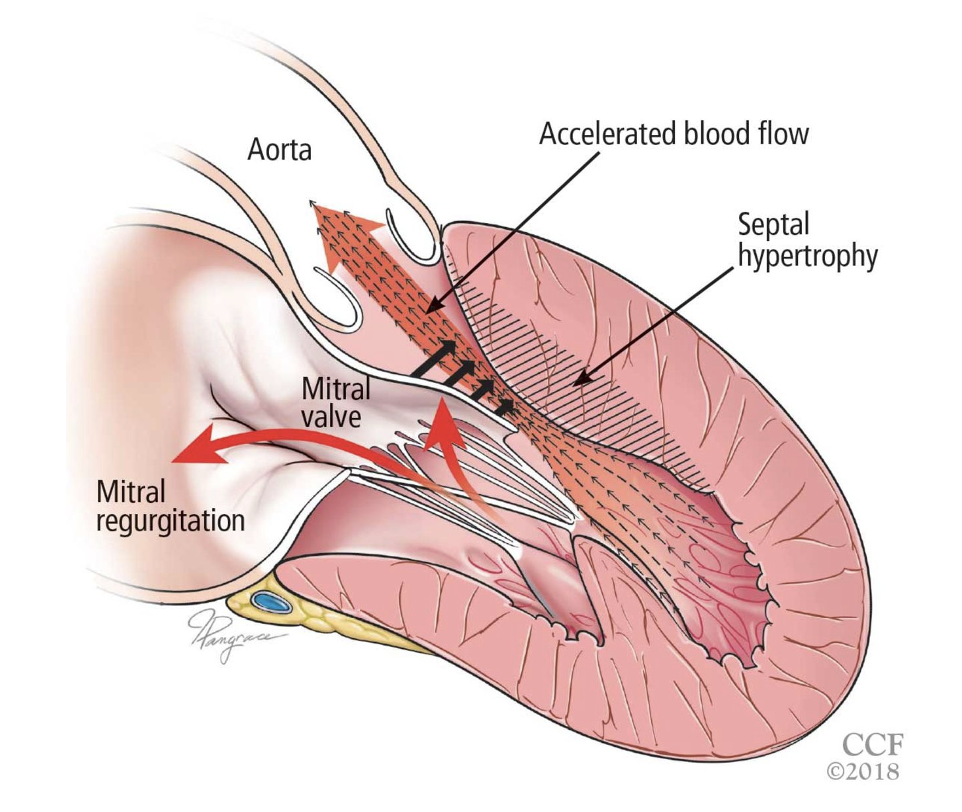
Before we delve into the ultrasound findings, let’s review the structural changes of the heart in HCM:
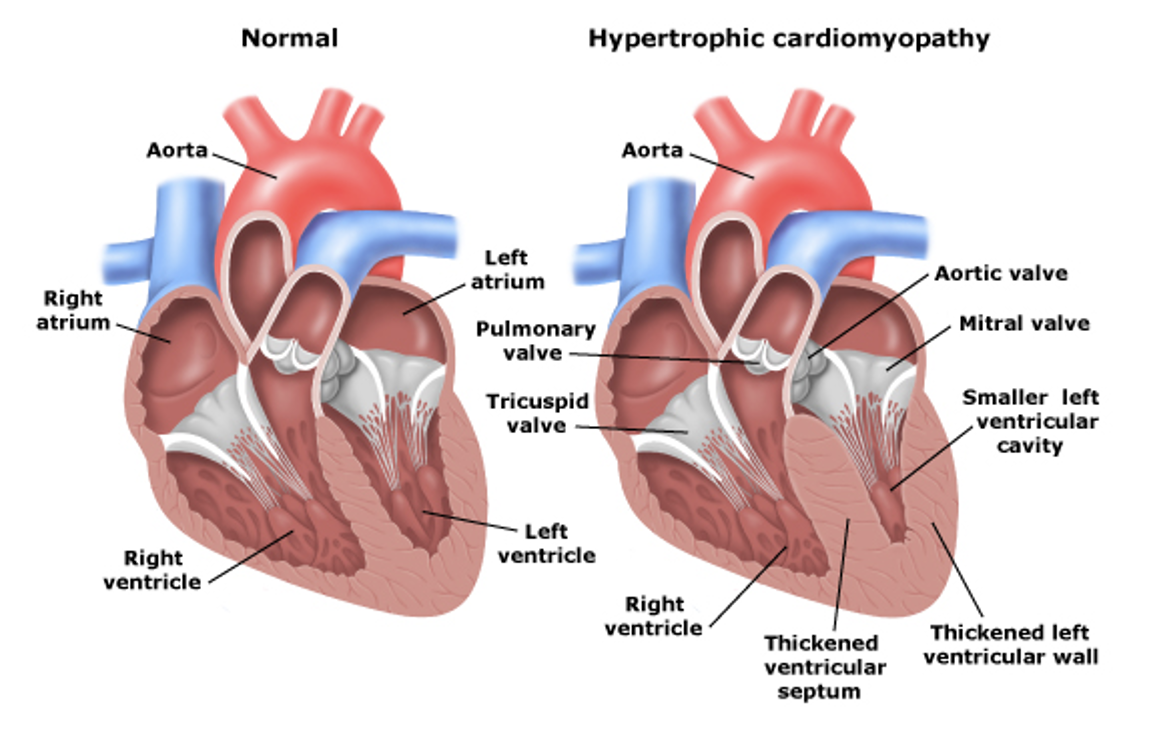
The 2 main structural changes that happen are:
1) Left Ventricular and Septal Wall Thickening
2) Interventricular Obstruction (aka LVOTO)
Now let’s POCUS!
These are the key POCUS findings in identifying HCM:
Unexplained LV wall thickening at any segment during diastole
Asymmetrical septal hypertrophy
Systolic anterior motion (SAM) of mitral valve
Left ventricular outflow tract obstruction (LVOTO)
ACEP created this great diagram that overviews these findings
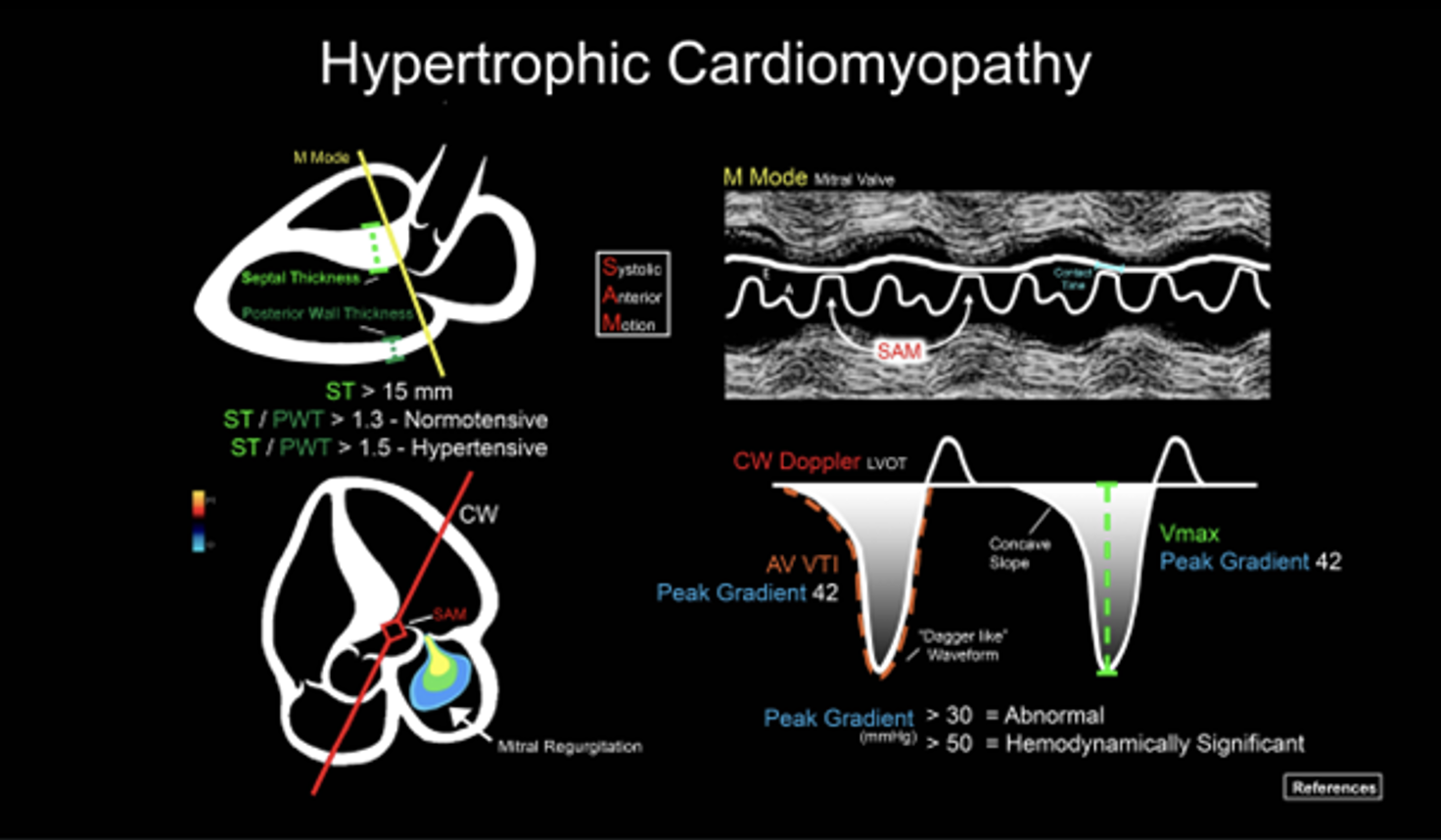
Finding #1: Unexplained LV wall thickness of > 15 mm at any segment during diastole
View: PSL View
“Unexplained” meaning not due to a history of longstanding hypertension, aortic stenosis, a highly competitive athlete, or other etiologies
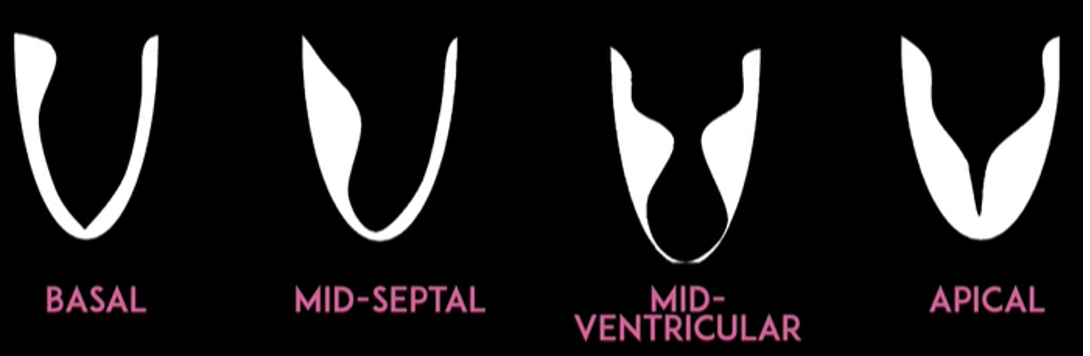
Typically there is focal thickening - can be basal, mid-septal, mid-ventricular, apical
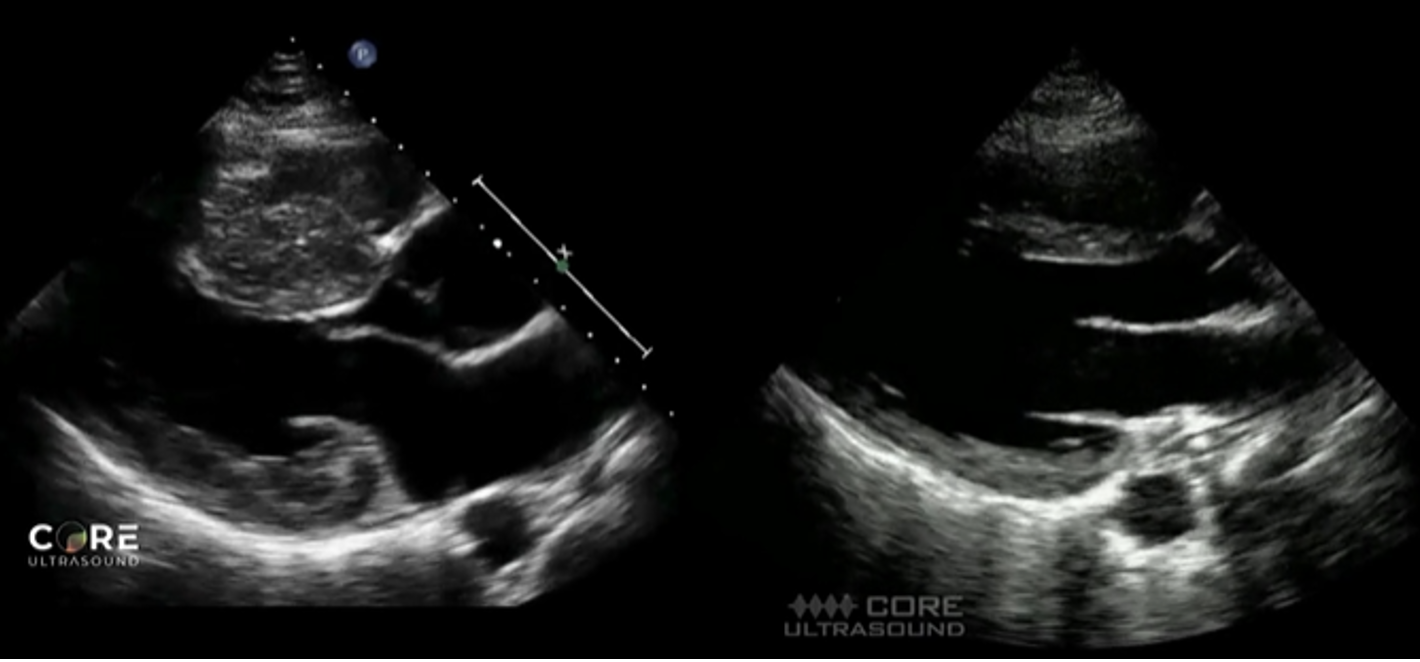
Left image shows septal and LV wall thickening, consistent with HCM. Right image is of a normal heart.
Finding #2: Asymmetrical septal hypertrophy
View: PSL or PSS View
Look for a ratio between the interventricular septum/posterior wall thickness
Ratio > 1.3 in normotensive patients is consistent with HCM
Ratio > 1.5 in hypertensive patients is consistent with HCM
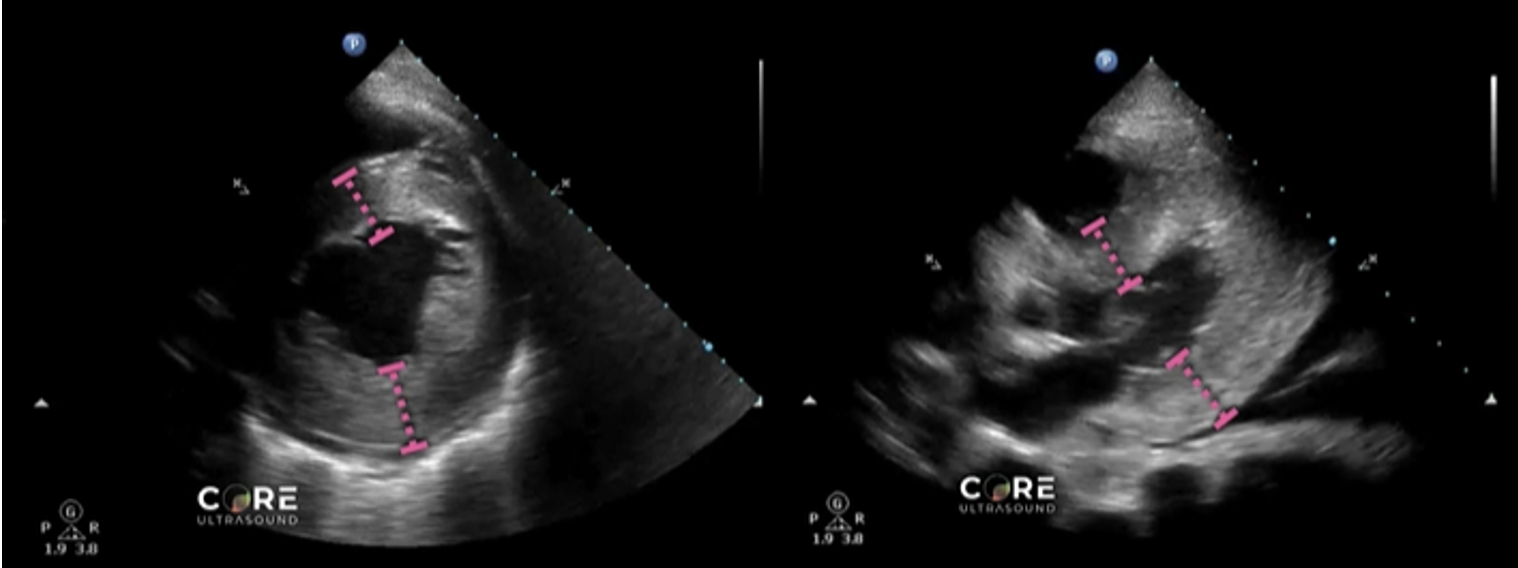
Left image shows how to measure the septal wall and LV wall in the PSS view. Right image shows the same in the PSL view.
Finding #3: Systolic anterior motion (SAM) of mitral valve
View: PSL View with M Mode, place axis as if you were measuring EPSS at tip of mitral valve
During systole, the mitral valve should be closed. But in HCM, the mitral valves actually move anteriorly during systole. This can be visualized by using M-Mode.
This finding used to be pathognomonic for HCM but recent studies have found that only 25-50% of HCM patients with SAM have LVOTO
The time the mitral valve is in contact with the septum can classify disease severity:
Mild: brief SAM without septal contact
Moderate: septal contact is < ⅓ of systolic period
Severe: septal contact is > ⅓ of systolic period
Notably, you will also see mitral regurgitation on ultrasound as well
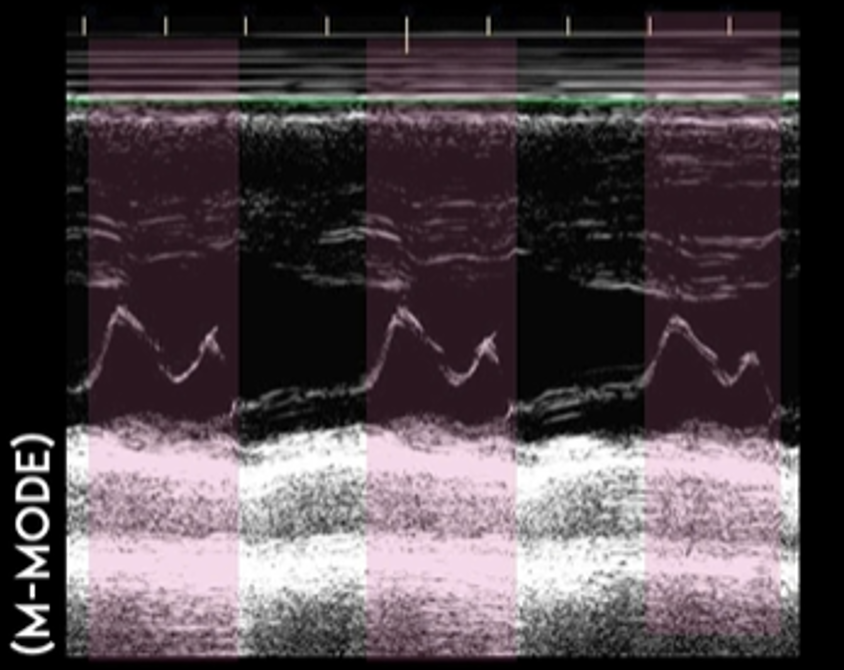
This is the M Mode on the PSL View of a normal heart. Notice how you see the opening of the mitral valve in diastole (almost touches the septum) and the closing of the mitral valve in systole.
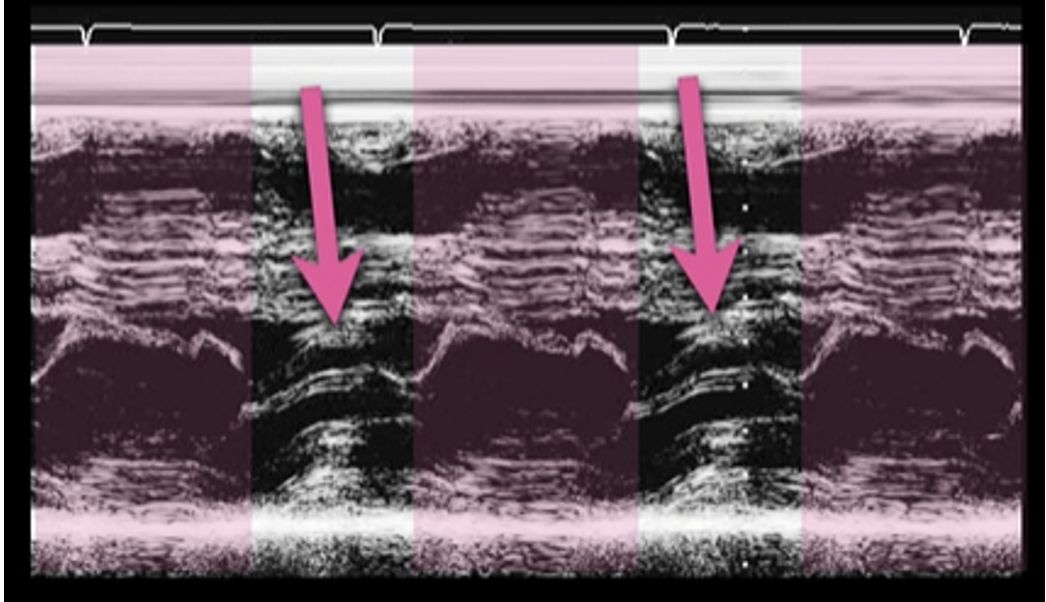
This is the M Mode on the PSL View of a heart with HCM. Notice how you see the opening of the mitral valve in diastole (valve touches the septum), BUT you see the mitral valve moving anterior during systole (arrows).
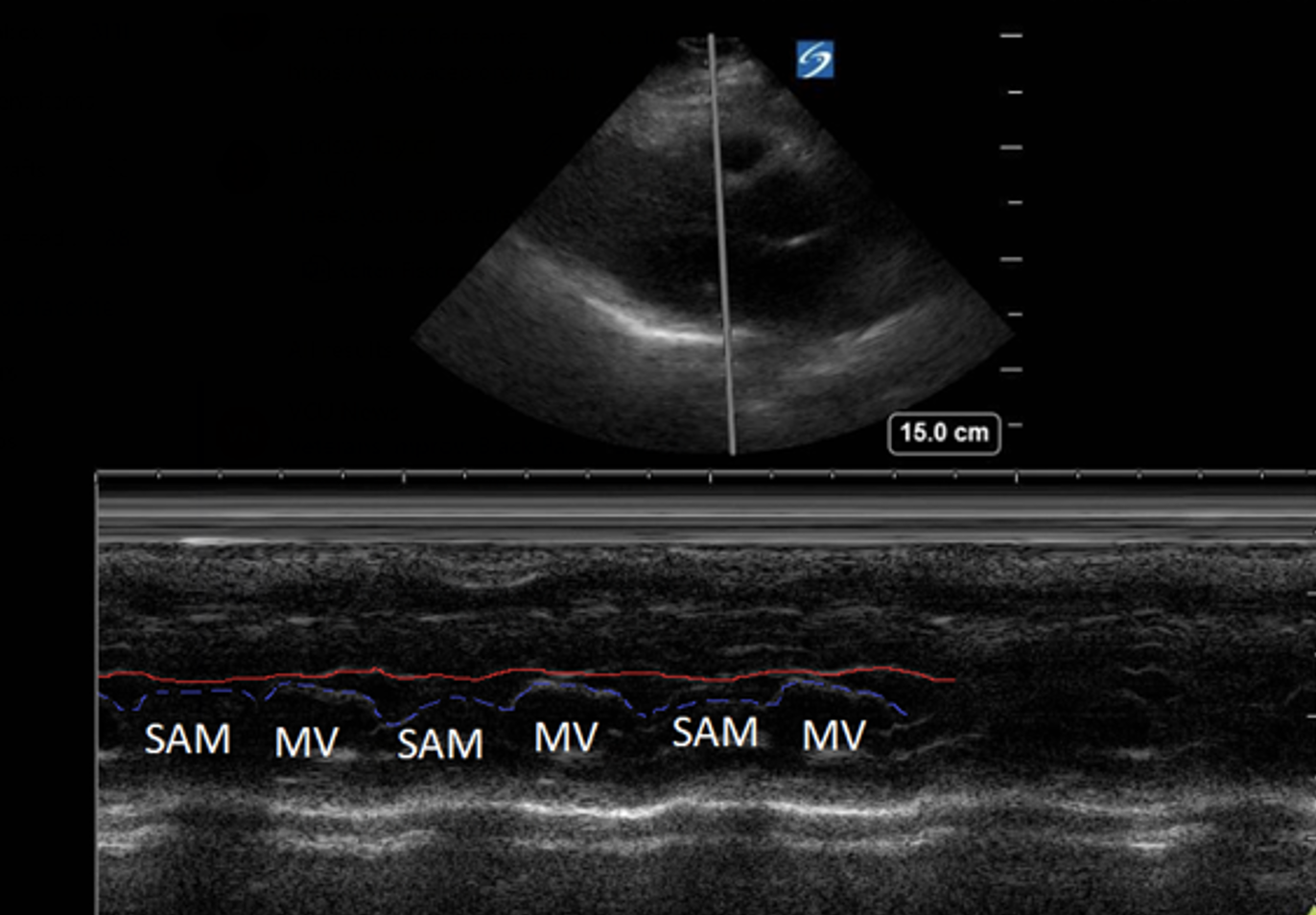
This is another example of SAM on a HCM patient.
Finding #4: Left Ventricular Outflow Tract Obstruction (LVOTO)
View: A5 View with Continuous Wave Doppler
Doppler will show “dagger-like/shark fin” waveform (produced by a late systolic peak)
Measure peak velocity to obtain a gradient
Gradient > 30 mmHg indicates obstruction
⅓ of HCM patient will have a high gradient at rest
⅓ of HCM patients will have a high gradient with provocation (Valsalva, exercise, medication)
⅓ of HCM patients will have no obstruction
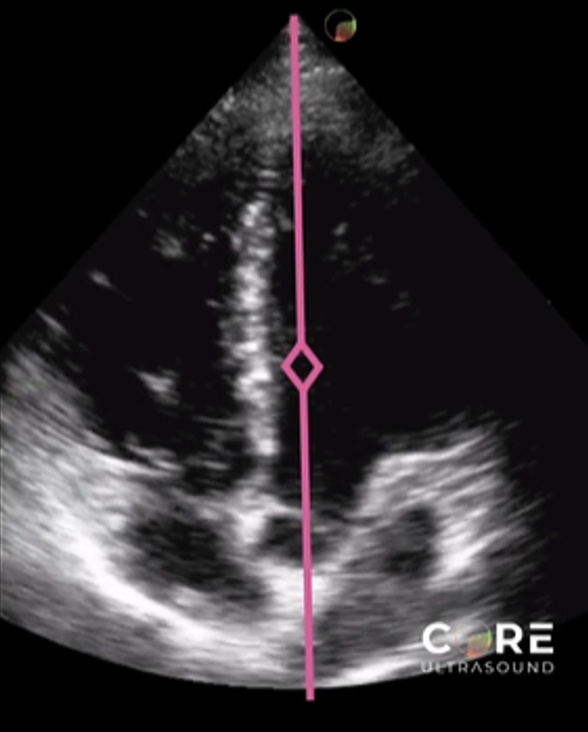
This is where you would place your Continuous Wave Doppler axis.
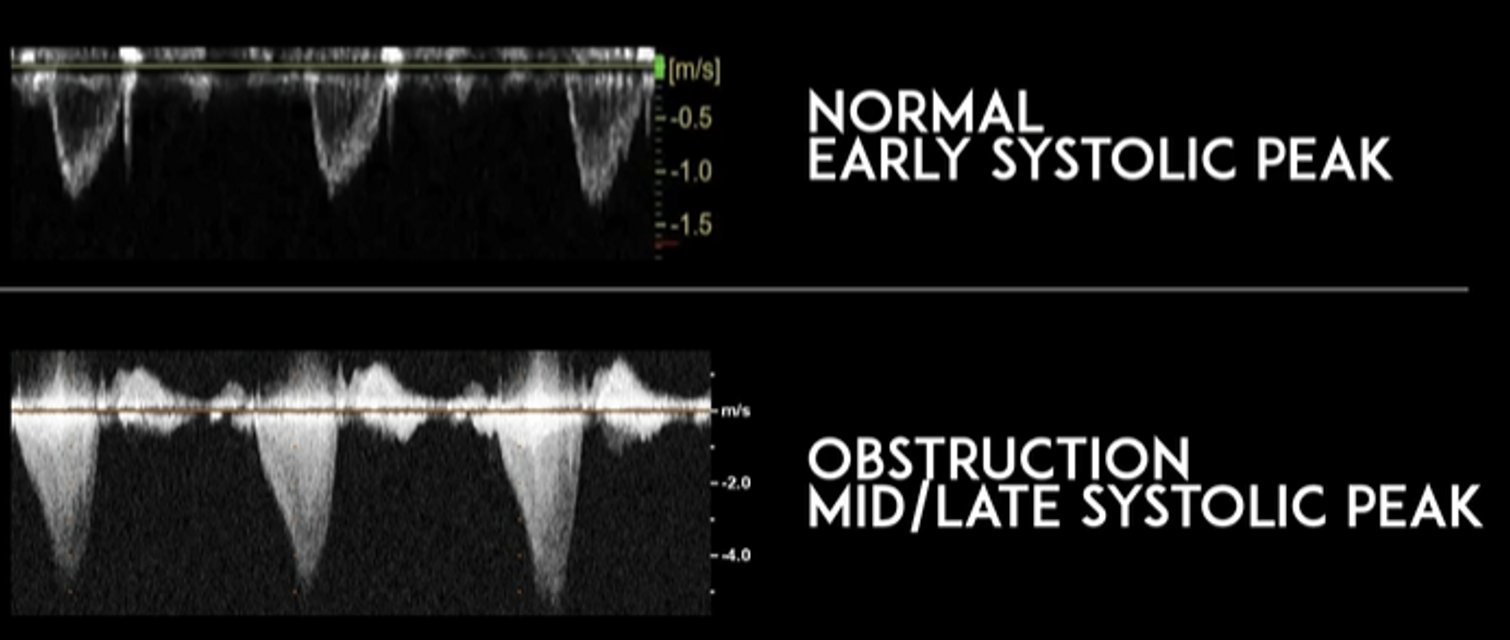
This image compares the waveforms of normal findings vs obstructive findings. Notice how the obstructive pattern appear like “daggers” or “shark fins.”
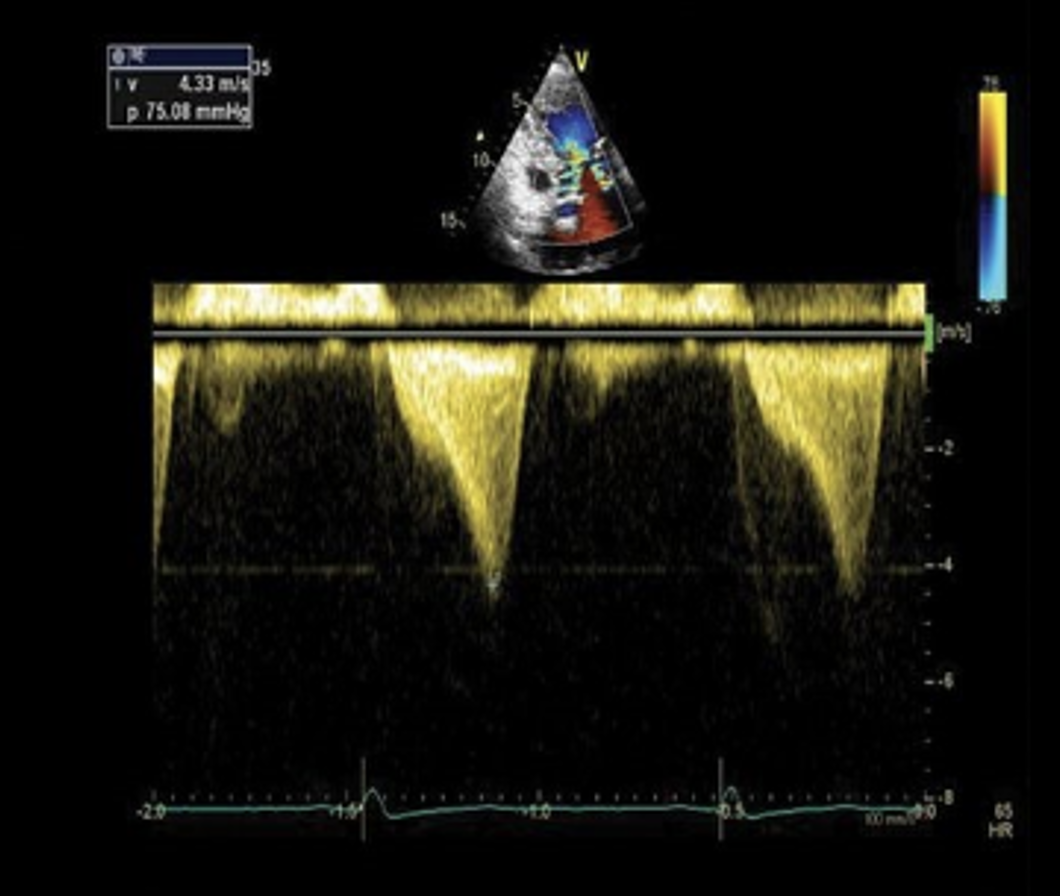
This is another example of the “dagger-like” waveform on a patient with HCM.
Diagnosis of HCM
Diagnosis is made by a formal echocardiogram or cardiac MRI showing LVH caused by no other etiology
Other considerations and workup supports this diagnosis:
Patient’s symptoms
Heart murmurs on exam
EKG
Genetic testing
These patients will require admission for further cardiac workup
Treatment of HCM
Depends on if the patient has obstructive or non-obstructive HCM
Patients are risk stratified for sudden cardiac death and are treated accordingly
Main treatments:
Beta blockers or calcium channel blockers to reduce heart rate
Pacemaker or ICD for ventricular arrhythmias
If patient fails initial treatments and has obstructive HCM, definitive treatment would be septal reduction therapy
Septal Myomectomy
Alcohol ablation or radiofrequency catheter ablation
Additional advisements:
Avoid physical activity, sports, or any exertion
Genetic counseling
Back to our patient… these were our bedside POCUS findings:
PSL View:
Based on our measurement, the interventricular septal-to-LV wall thickness ratio would be 16.5 mm/32.5 mm = 0.51. This is not consistent with HCM. However, the LV wall thickness is 32.6mm, which would be consistent with HCM.

We used M Mode on the mitral valve and did not see SAM.
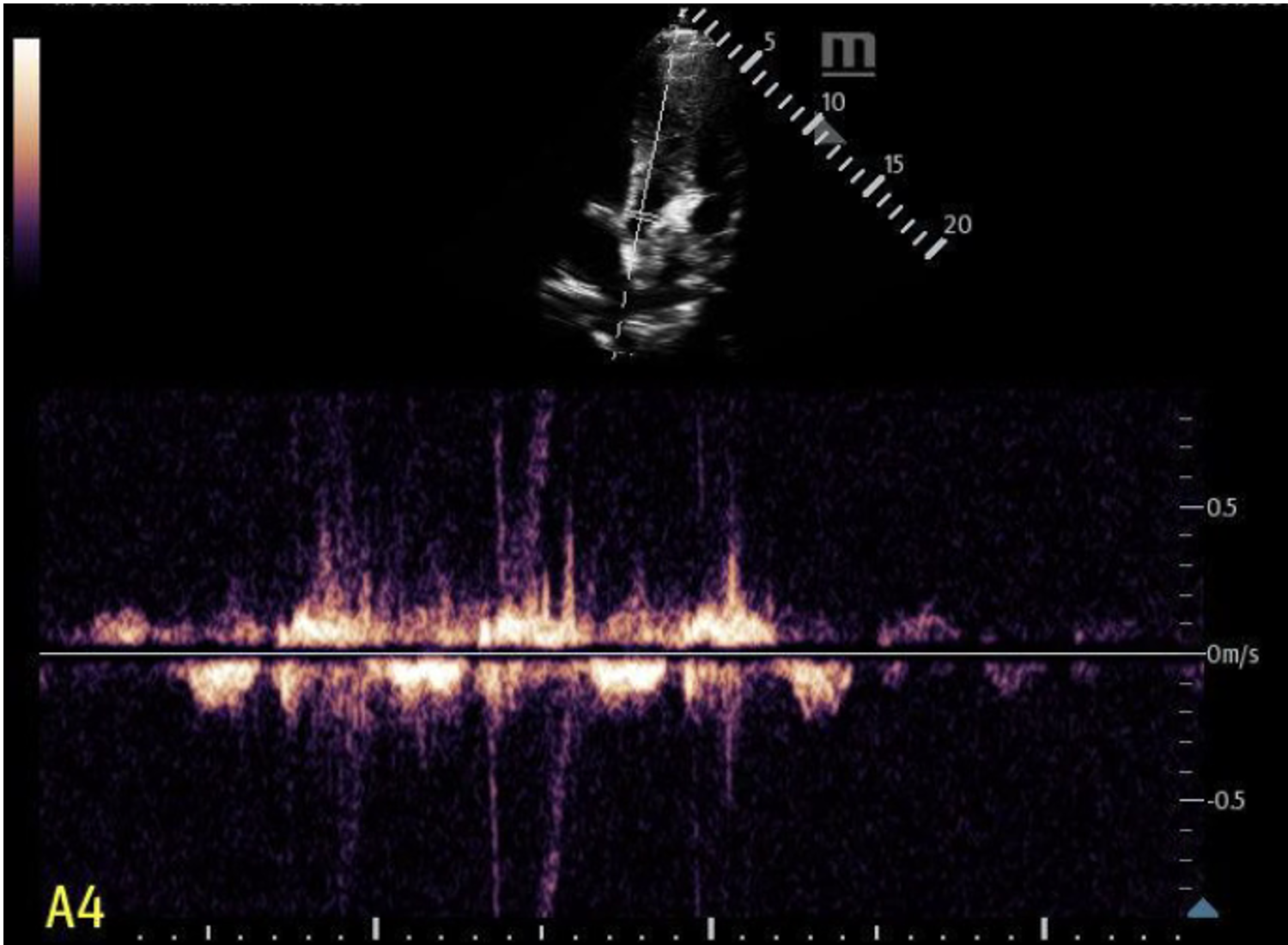
We used continuous wave doppler in a limited A5 view. We did not see any obvious “dagger-like” or “shark fin” waveforms.

The rest of the patient’s hospital course:
Formal echo showed: Mild concentric LV hypertrophy, particularly in the apex and free wall measuring up to 15 mm. No LVOTO. Mild mitral valve insufficiency. Mild aortic insufficiency. Normal coronary artery origins. Thickened and hypertrophied mitral valve papillary muscles. LV diastolic dysfunction. Normal LV systolic function.
Pediatric cardiology was consulted and recommended transfer to Cornell. Patient was admitted for telemetry and further cardiac workup, including Holter monitor, cardiac MRI, and genetics evaluation.
Patient was ultimately discharged a couple of days after admission with a Zio Patch for 5 days, was prescribed Amlodipine, and scheduled outpatient followup with cardiology.
Summary of HCM POCUS:
Unexplained LV wall thickening of > 15 mm at any segment during diastole
Asymmetrical septal hypertrophy
Interventricular septal wall/LV wall thickness with ratios of:
> 1.3 in normotensive patients
> 1.5 in hypertensive patients
Use M Mode to check for systolic anterior motion (SAM) of mitral valve
Use continuous wave doppler in the A5 view to check for left ventricular outflow tract obstruction (LVOTO), where gradient is > 30 mmHg
Happy scanning!
Resources
Avila J. 5 Minute Sono: HCM and LVOTO (2024) - Core Ultrasound. Core Ultrasound - free and subscription ultrasound education for medical professionals. Published August 12, 2024. https://coreultrasound.com/5-minute-sono-hcm-and-lvoto-2024/
Buttner R, Burns E. Hypertrophic Cardiomyopathy (HCM) • LITFL • ECG Library Diagnosis. Life in the Fast Lane • LITFL • Medical Blog. Published March 16, 2019. https://litfl.com/hypertrophic-cardiomyopathy-hcm-ecg-library/
Fischer K, Taylor L. Motion of the HOCean: A Clinical Case of Hypertrophic Obstructive Cardiomyopathy (HOCM). www.acep.org. Published January 20, 2023. https://www.acep.org/emultrasound/newsroom/jan2023/motion-of-the-hocean-a-clinical-case-of-hypertrophic-obstructive-cardiomyopathy
Stoll CM, Carr M, Naraghi L. Hypertrophic Cardiomyopathy Diagnosed on Point-of-Care Echocardiogram in an Elderly Patient With Syncope. Cureus. Published online August 8, 2021. doi:https://doi.org/10.7759/cureus.17008