
To PE or not to PE, That is the Question
Written by: Dr. Marlene Louro
Edited by: Dr. Joann Hsu
The case:
HPI: 77 yr old F w/ PMH of CAD, breast cancer s/p lumpectomy, htn, hld presents to the ED w/ one week of chest pain and shortness of breath. She endorsed lower right pleuritic chest pain that worsened with coughing. It then progressed to acute onset dyspnea, which prompted her ED visit. Denies recent prolonged immobilization, surgery or trauma.
Vital Signs: BP: 133/82, tachycardic to 116, hypoxic to 91% on RA and 96% on 2L NC, RR:18
Pertinent Physical Exam: Lungs clear to auscultation bilaterally, +2 pitting edema in lower extremities bilaterally, otherwise normal
POCUS time:
Initially, the clinical picture seemed to fit infectious etiology (pneumonia or viral URI) or possibly CHF, but let’s get the probe on the patient to help guide our differential.
In the parasternal long view, the right ventricular outflow tract (RVOT), aortic root and left atrium should all be about equal in size (rule of thirds), however the RVOT looks enlarged in comparison.
In the parasternal short view, notice that the right ventricle is enlarged compared to the left ventricle. Also, there is bowing of of the interventricular septum during diastole, aka “D sign” — this is concerning for right heart strain.
In the apical 4 chamber view, again demonstrated is the dilated right heart concerning for right heart strain.
When looking at the Apical Four Chamber view, how can you confirm that you’re actually looking at the RV and don’t have the probe marker flipped?
Tricuspid valve tends to be more near field than the mitral valve
Moderator band may be seen in the right ventricle
In the apical 5 chamber view, can see the LVOT located in the LV
Why is acute right heart strain in the setting of a PE scary?
Pulmonary Embolism Spiral of Death!!
In a pulmonary embolism, this is caused by obstruction of the pulmonary vasculature leads to a sudden increase in pulmonary vascular resistance.
This places an acute pressure overload on the right ventricle (RV), which must work harder to maintain forward flow.
As the RV struggles, it dilates and begins to shift the interventricular septum toward the left ventricle (LV), impairing LV filling and reducing cardiac output.
The resulting decrease in systemic perfusion exacerbates RV ischemia, as the RV relies on both systolic and diastolic perfusion—both of which are compromised in this setting.
This vicious cycle leads to worsening RV failure, hypotension, and ultimately cardiogenic shock.
Without prompt intervention, rapid clinical deterioration can occur.
What should you do if you are suspicious that a patient may have a PE and you notice signs of right heart strain on bedside echo?
Act quickly! Get the patient on a monitor and push to get the CTA as quickly as possible.
Right heart strain on echo could indicate impending hemodynamic instability
How can we classify our patient’s PE? Let’s look at the different classifications of PE:
Massive: Acute PE with sustained hypotension (systolic blood pressure <90 mm Hg for at least 15 minutes or requiring inotropic support, not due to a cause other than PE.
Submassive: Acute PE without systemic hypotension (systolic blood pressure ≥90 mm Hg) but with either RV dysfunction or myocardial necrosis. RV dysfunction (on echo) described as: RV dilation or RV systolic dysfunction.
Low Risk PE: Acute PE, normotensive with normal biomarker levels and no RV dysfunction on imaging.
It is important to note that RV dilation and D sign can also be seen in chronic heart strain and is not specific for acute right heart strain!!!!
What are some causes of chronic right heart strain?
Pulmonary Hypertension
COPD
Interstitial lung disease
Obstructive Sleep Apnea
How can you differentiate chronic vs acute right heart strain?
RV hypertrophy (>5mm in subxiphoid view during diastole)
McConnell’s sign
60/60 sign
Early Systolic Notching
This is a big topic for another day.
Now, let’s add some numbers to this and talk about TAPSE:
What does it stand for?
Tricuspid Annular Plane Systolic Excursion
What is it?
It is an assessment of the global systolic RV function.
It measures the distance that the RV annular segment moves longitudinally during contraction.This correlates with RV ejection fraction since the RV does not contract concentrically like the LV does.
How to find TAPSE?
Obtain Apical 4 Chamber view, making sure you are able to completely see the right ventricle.
Turn on M-Mode and place the cursor at the tricuspid annulus.
Measure the distance from peak to trough, which represents the distance the annulus moves from its end-diastolic position to its maximum systolic position.
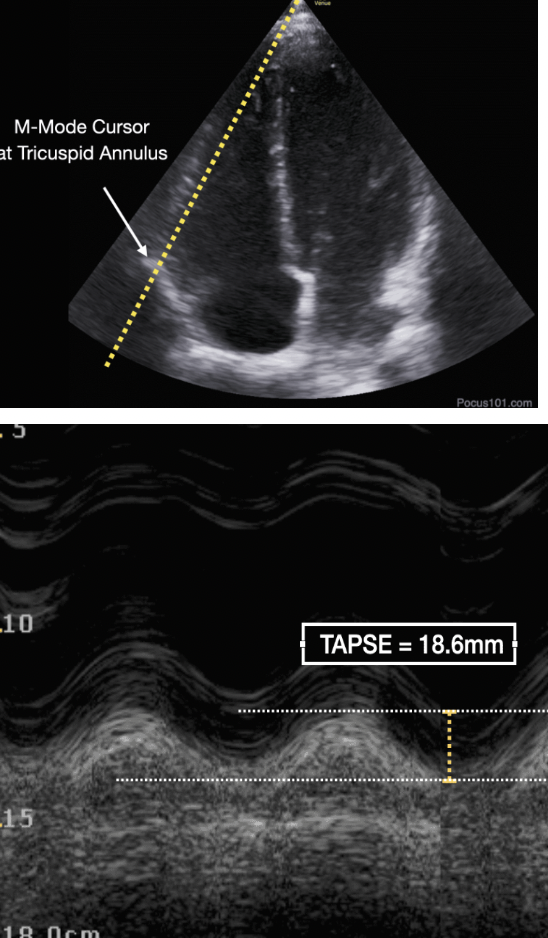
How do you interpret TAPSE?
If TAPSE is greater than 16mm, that indicates normal right ventricular function.
If TAPSE is less than 16mm, it suggests there is right ventricular systolic dysfunction. This can be seen in the setting of PE as well as chronic processes such as pulmonary hypertension, right ventricular MI, etc.
Why is TAPSE important in acute PE?
TAPSE is used for risk stratification
In PE, TAPSE has been found to be an independent predictor of in hospital mortality or thrombolysis.
The study by Pruszczyk et al. (2014), found that in normotensive patients with acute PE, TAPSE ≤15 mm identifies patients with an increased risk of 30-day APE-related mortality. TAPSE >20 mm can identify very low-risk group.
Back to our patient:
CT pulmonary angiography revealed an acute pulmonary embolism involving the left main pulmonary artery as well as bilateral lobar, segmental, and subsegmental branches. Imaging also demonstrated signs of mild right heart strain, consistent with findings from our bedside echo.
Laboratory workup was notable for elevated D-dimer, troponin, and BNP levels. A formal echo showed a TAPSE of 19 mm, suggesting preserved right ventricular function and a low 30-day mortality risk.
The patient was diagnosed with intermediate high risk PE, and both the MICU and CCU teams were consulted. She was not a candidate for catheter-directed thrombolysis (CDT) or surgical thrombectomy. Ultimately, she was admitted to the medical floor and initiated on intravenous heparin for anticoagulation.

Takeaways of this case:
Do a bedside echo on all patients you suspect may have a PE.
If signs of right heart strain are present on echo in a normotensive patient and clinical suspicion for PE is high, escalate care promptly. Place the patient on continuous monitoring and obtain a STAT CTA, as these patients can decompensate rapidly.
Happy Scanning!
References
Jaff, M. R., McMurtry, M. S., Archer, S. L., Cushman, M., Goldenberg, N. A., Goldhaber, S. Z., ... Zierler, B. K. (2011). Management of massive and submassive pulmonary embolism, iliofemoral deep vein thrombosis, and chronic thromboembolic pulmonary hypertension: A scientific statement from the American Heart Association. Circulation, 123(16), 1788–1830. https://doi.org/10.1161/CIR.0b013e318214914f
Jailyn. (2020, February 14). 5 Min Sono – Right Heart Function. Core Ultrasound. Retrieved September 7, 2025, from Core Ultrasound website: “5 Min Sono – Right Heart Function”
Krishtopaytis, E., Johnson, A., Pant, S., & Dinh, V. (n.d.). Right ventricular ultrasound – qualitative and quantitative assessments. POCUS 101. Retrieved September 7, 2025, from POCUS 101 website: “Right Ventricular Systolic Pressure (RVSP)” section
Pruszczyk, P, Goliszek, S, Lichodziejewska, B. et al. Prognostic Value of Echocardiography in Normotensive Patients With Acute Pulmonary Embolism. J Am Coll Cardiol Img. 2014 Jun, 7 (6) 553–560.
https://doi.org/10.1016/j.jcmg.2013.11.004
Weekes AJ, Thacker G, Troha D, Johnson AK, Chanler-Berat J, Norton HJ, Runyon M. Diagnostic Accuracy of Right Ventricular Dysfunction Markers in Normotensive Emergency Department Patients With Acute Pulmonary Embolism. Ann Emerg Med. 2016 Sep;68(3):277-91. doi: 10.1016/j.annemergmed.2016.01.027. Epub 2016 Mar 11. PMID: 26973178.