
Breakin’ My Heart
Written by: Dr. Eugene Borst
Edited by: Dr. Joann Hsu
Case Presentation
A 66 yo female, with a PMH of HTN, HLD, A-Fib s/p ablation (not on AC), former smoker, presented to the ED for evaluation of left sided chest pain described as crushing pain that radiated to the left shoulder. She stated that the pain was intermittent for the past 3 days with an association of chest discomfort. About 1 hour prior to arrival, she was taking a shower when she had sudden worsening of her left sided chest pain that was persistent and associated with nausea.
Vitals: BP 110/70, T 36.6, RR 15, HR, 111, SPO2 sat at 97% on RA
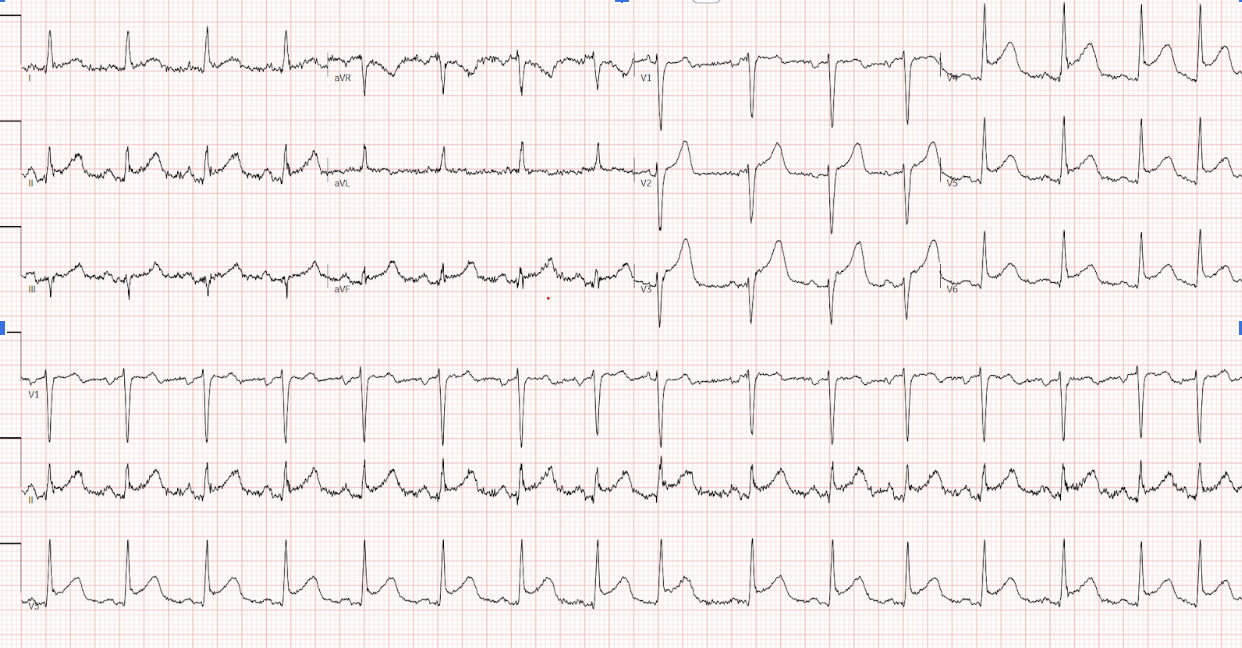
Labs: troponin 166. EKG shown below.
Bedside POCUS
There was inferolateral wall motion abnormality, basal hypercontractility, apical ballooning
No pericardial effusion.
Here are the POCUS images:
Hospital course
The patient was taken to the cath lab for Left Heart Catheterization (LHC) and admitted to the Coronary Care Unit (CCU).
LHC showed no coronary blockage and apical ballooning of the left ventricle, consistent with the diagnosis of Takotsubo cardiomyopathy. Transthoracic Echo (TTE) was done post catheterization. Summary of findings shown below.

Takatsubo Cardiomyopathy
This is also known as stress-induced cardiomyopathy or “broken heart syndrome.”
It is described as a transient regional wall motion abnormality or left ventricle systolic dysfunction that mimics an acute MI in EKG changes and clinical presentation.
Key features required for diagnosis:
Transient hypokinesis, akinesis, or dyskinesis in the left ventricular mid segments with or without apical involvement; regional wall motion abnormalities that extend beyond.
A single epicardial vascular distribution and frequently, but not always, a stressful trigger.
The absence of obstructive coronary disease or angiographic evidence of acute plaque rupture.
New ECG abnormalities (ST-segment elevation and/or T-wave inversion) or modest elevation in cardiac troponin.
The absence of pheochromocytoma and myocarditis.
This POCUS finding may also be described as systolic apical ballooning of the LV with hyperkinesis of the basal walls. Of note, there are also less common regional wall motion abnormalities seen.
The key in this diagnosis is that there is NO evidence of obstructive CAD or plaque rupture on coronary angiography.
For this reason, this diagnosis cannot be definitively made based on POCUS findings or in the emergency department.
However, this is a very interesting sonographic finding and one that could clue you in on possible stress-induced cardiomyopathy while working the patient up in the ED.
Happy scanning!
References
https://www.ncbi.nlm.nih.gov/books/NBK430798/