
WRAPplication of ACCENT protocol
Written by: Dr. Thomas Sanchez
THE CASE:
30 year old female with a history of s/p C-sections x 2, presents for RLQ abdominal pain since last night. Patient states that at 11 PM she started to feel nagging pain to RLQ of abdomen. Endorses association of dysuria, as well as radiation of pain to the back and groin from RLQ. Denies ever having pain like this before. Denies nausea, vomiting, diarrhea, or fevers. Notes pain is constant, worsening with movement and walking.
Physical Exam:
Patient is awake, alert, and in no acute distress.
SKIN: Warm, dry; (-) cyanosis; (-) rash.
HEAD: (-) scalp swelling, (-) tenderness.
EYES: (-) conjunctival pallor, (-) scleral icterus, (+) EOMI
ENMT: Pharynx: (-) erythema; airway patent: (-) stridor; mucous membranes moist.
NECK: (-) tenderness, (-) stiffness
CHEST AND RESPIRATORY: (-) rales, (-) rhonchi, (-) wheezes; breath sounds equal bilaterally.
HEART AND CARDIOVASCULAR: (-) irregularity; (-) murmur, (-) gallop.
ABDOMEN AND GI: Soft; (-) guarding, (-) rebound, (-) Murphy's, (-) McBurney's. (+) RLQ tenderness
EXTREMITIES: (-) deformity, (-) edema, (-) tenderness, (+) full range of motion, (+) equal pulses in upper and lower extremities
A/P:
Differentials include but not limited to appendicitis vs pyelonephritis vs nephrolithiasis vs ovarian torsion vs other acute pathology. Will order labs, endovaginal US, and CTAP with IV contrast.
Wow, that’s a bunch of interesting differentials!
Women with right sided abdominal pain are suspicious for a wide range of pathologies.

Thankfully, a lot of them can be looked for and even ruled out at the bedside with your trusty POCUS!
At NYPQ, we are developing a protocol for evaluation of these pathologies. WRAP (Women with Right Abdominal Pain)
Appendicitis
Cholecystitis
Cyst (Ovarian)
Ectopic Pregnancy
Nephrolithiasis
Torsion (Ovarian)
What images were we able to obtain from our patient?
A
Appendicitis - Does not look like there is a huge closed off tube to represent an inflamed appendix in this clip!
C
Cholelithiasis - Also, looks ok here. No gallstones in this clip.
Further, no signs of cholecystitis
No Gallbladder wall thickening
No Pericholecystic fluid
No Gallbladder hydrops
No stone in the Gallbladder neck
*Reported No sonographic Murphy’s sign*
No dilation of CBD
C
Cyst (Ovarian) - Hmm, something is here
There is a complicated structure visible.
Described as an ovoid cystic lesion with lobular contour and nodular septae
Maybe this is what is causing the pain! A ruptured ovarian cyst!
But, we should keep looking, can never be sure the patient does not have something more dangerous.
E
Ectopic pregnancy - There is definitely a structure here, but this is the same cyst we saw
Since it is INSIDE the Ovary, seems less likely to be a pregnancy. No gestational sac or other features of pregnancy here.
Keep in mind this information needs to be analyzed in conjunction with other objective findings, such as HCG level, whether via urine or blood.
N
Nephrolithiasis - Great images!
No hydronephrosis seen!
They also confirmed that the hypoechoic areas were vascular and not signs of hydronephrosis using color flow.
Further, no hyperechoic structures visualized that could represent intrarenal or intrapelvic stones.\
T
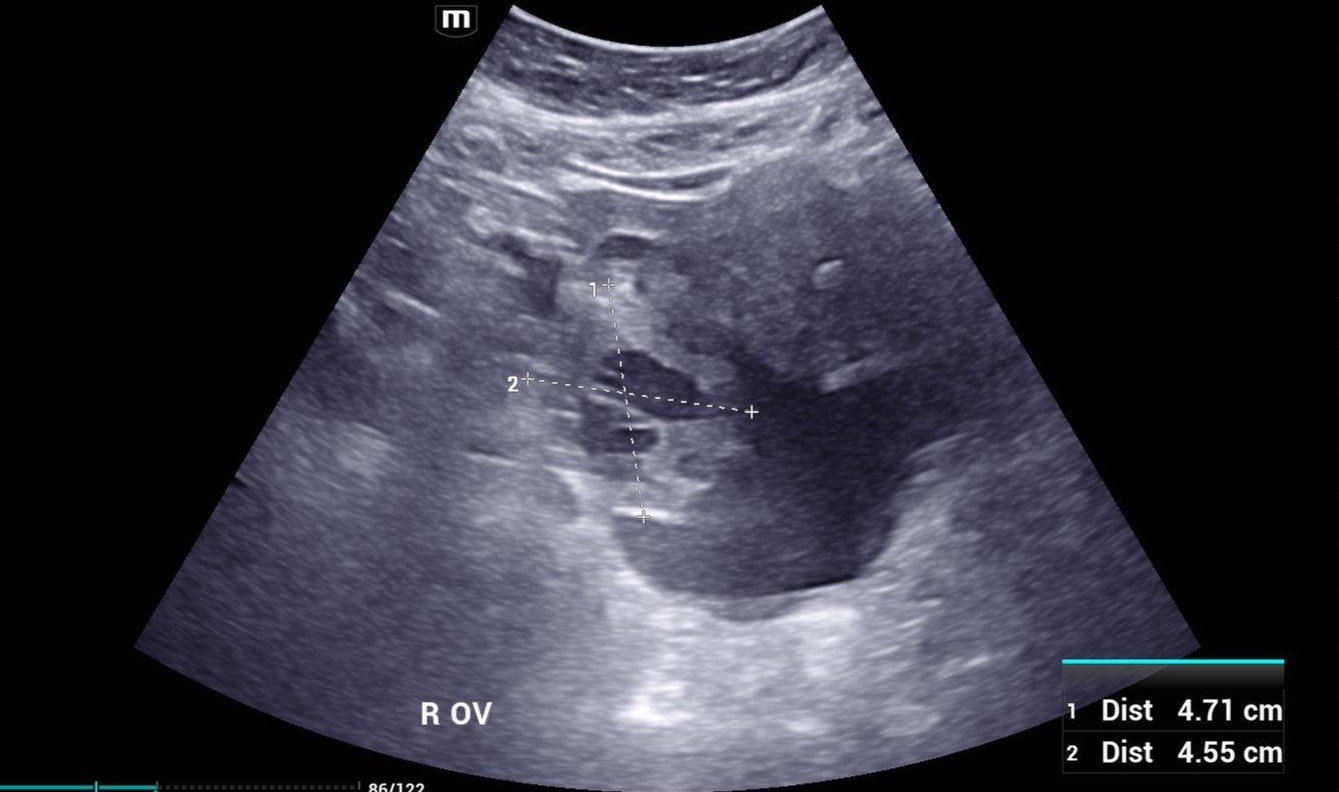
Torsion - Complex structure still here
With more images of the complex structure in the right adnexa, we get a clearer picture of the pathology.
Torsion can be identified acutely on US by measuring resistive index. Though that is quite difficult here given the complex cyst within. Cysts typically have to be at least 5cm large to create a nidus for rotation and make the ovary torse.
Seen here, the whole ovary is being measure at 4.7 cm wide, which means it is not big enough by usual standards. If the story added up to torion, it should still be considered, but this patient’s story fits more with a ruptured cyst. And there is some small amount of fluid in the pelvis, which is likely from this ruptured ovarian cyst.
Remember for your Boards and ITE that the most common finding on US for a patient with ovarian torsion is enlargement of the ovary!
Great, we did the protocol! Seems like ruptured cyst is the most likely explanation for this patient’s pain. What did her workup demonstrate?
Official Ultrasound Results
Right ovarian complex 3 cm cystic lesion, possible evolving hemorrhagic cyst.
CTAP Results
1. Right adnexal 2.8 cm cyst, most likely a luteal cyst.
2. Fluid in the pelvis, and trace fluid more superiorly; most likely at least partly hemorrhage, and very likely due to ruptured