
Then I took a POCUS to the KNEE
Written by: Dr. Thomas Sanchez
THE CASE:
65 yo M w no pmhx presents complaining of sudden onset left knee pain that he woke up with in the morning. He denies any trauma. States there is intermittent pain when, especially he bends his knee, which has been causing him pain sometimes when he walks. Denies any other symptoms, states this has never happened before.
Physical Exam:
Vitals within normal limits.
Left knee without any edema or erythema. There is mild tenderness to palpation in the popliteal fossa. Active and passive range of motion intact.
Imaging:


No acute osseous abnormalities identified.
So let’s get our handy-dandy… Ultrasound probe.
As it turns out, Ultrasound is pretty good aty identifying soft tissue injury, even when compared to MRI! https://pubmed.ncbi.nlm.nih.gov/34851172/
But, as always, this is operator dependent! So you need to practice and know what you are looking at. Before we head over to the patient with our probe, we have to review.
You can use a linear probe or curvilinear probe. The linear will show you structures very clearly, so it may be better to showcase those injured soft tissues, but not every patient or pathology is the same.

What will we even be looking at? What are we looking for?


there are a lot of structures in there! We start holding the probe longitudinally above and below the knee
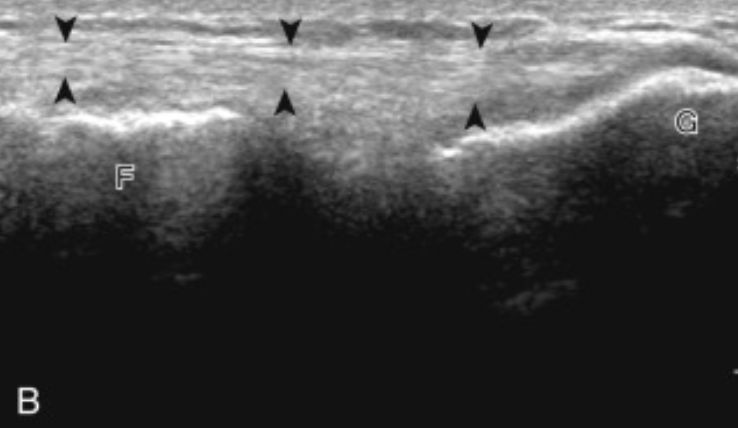
Suprapatellar View

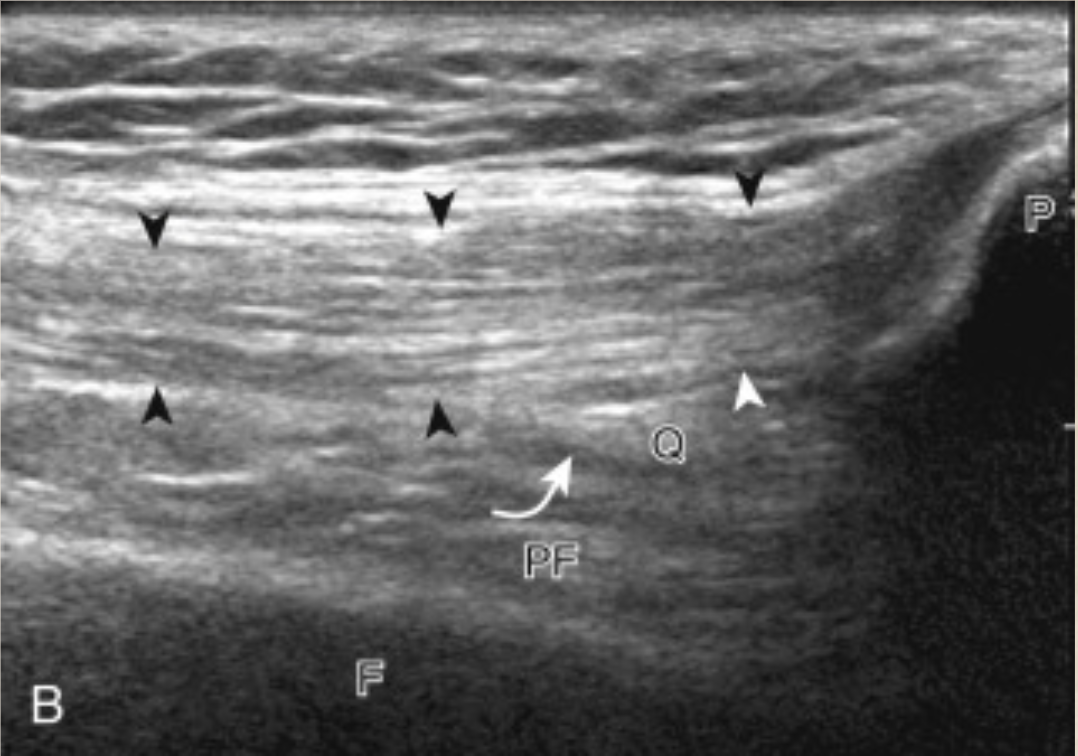
Infrapatellar View
The arrows delineate the quadriceps tendon
F is femur
P is patella
T is tibia
PF is prefemoral fat pad
Q is quadriceps fat pad
H is hoffa fat pad
Next we move the probe to the medial and lateral sides

Medial View!
Curved arrow is the Meniscus
The other arrows delineate the… MCL!
Lateral View! The arrows are pointing out the… LCL!
Here are images of our patient!
Suprapatellar^ Ignore the labels under the images! They were entered incorrectly. Hopefully you can make out the structures here, as detailed above. Infrapatellar^
Medial View^ Think these clips of the collateral ligaments look abnormal? Me too. This patient probably needs further imaging with an MRI. Lateral View^
But do meniscus injuries fit well with his clinical picture? Not perfectly. What else can we look for?
Included above was an image of the bursas of the knee. Bursitis can often be seen and is obvious, as there will be a large fluid collection. But it is harder to remember to look EVERYWHERE!

Prepatellar Bursitis

Infrapatellar Bursitis
Our patient did not have these, but there is one last hiding spot for pathology… The posterior!

Baker’s Cyst!
This patient had a Baker’s Cyst, too! So multiple reasons to refer to outpatient Orthopedics. We can give him some oral analgesia for home and put a nice wrap on his knee to keep some pressure on it. Ultrasound for the win!
Sources:
Our own clips!
https://pubmed.ncbi.nlm.nih.gov/34851172/
https://radiopaedia.org/cases/prepatellar-bursitis-2?lang=gb for images
https://www.pocus101.com/ultrasound-machine-basics-knobology-probes-and-modes/ for images
https://www.hopkinsmedicine.org/health/conditions-and-diseases/patellar-tendonitis-jumpers-knee for images
https://www.hirslanden.com/en/international/disease-patterns.disease.html/baker-zyste.html for images