
It's not Sci-Fi, its Pop-Sci
Written by: Dr. Haroon Karabay
Edited by: Dr. Joann Hsu
The case:
50 y.o f with no PMH presenting to the ED for right ankle pain. She was walking outside when she slipped on a patch of ice and inverted her right foot. She has been unable to walk since the incident.
Vitals: T 98.5F RR 24 HR 110 BP 137/78
Physical Exam:
On inspection of the right ankle, there is visible edema of the bilateral distal malleolar regions with tenderness to palpation. There is a normal sensation to light touch and the patient is able to spread their toes.
You being an astute physician decide to get an XR:

Findings of acute bilateral malleolar fracture
The patient received multiple rounds of pain medications in the Emergency Room while awaiting reduction by the orthopedic team. Given continued pain, a decision was made to perform a Popliteal Sciatic nerve block for better patient comfort.
The Popliteal Sciatic Nerve Block
The Popliteal Sciatic nerve block, also known as the distal sciatic nerve block, is a valuable technique that results in anesthesia of the calf, tibia, fibula, ankle, and foot.
The sciatic nerve consists of two separate nerve trunks: the tibial and common peroneal nerves. A common paraneural sheath envelops these two nerves from their origin in the pelvis.
As the sciatic nerve descends toward the knee, the two components eventually diverge just proximal to the popliteal fossa, giving rise to the tibial nerve (TN) and common peroneal nerve (CPN).
This division of the sciatic nerve usually occurs between 50 and 120 mm proximal to the popliteal fossa crease.
It is recommended to perform the nerve block at the level where TN and CPN start diverging but are still in the common sciatic nerve sheath.
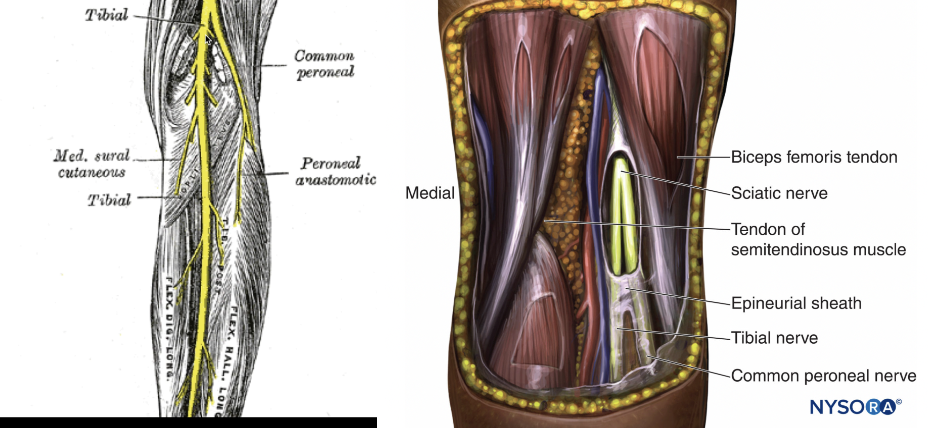

Red highlighted region indicates the anatomy that will be anesthetized when the block is performed correctly.
After obtaining informed consent and rounding up materials required for the procedure, you will then need to find the relevant anatomy of your patient with the use of the linear probe on the ultrasound machine.
Can be done by posterior approach or lateral approach.

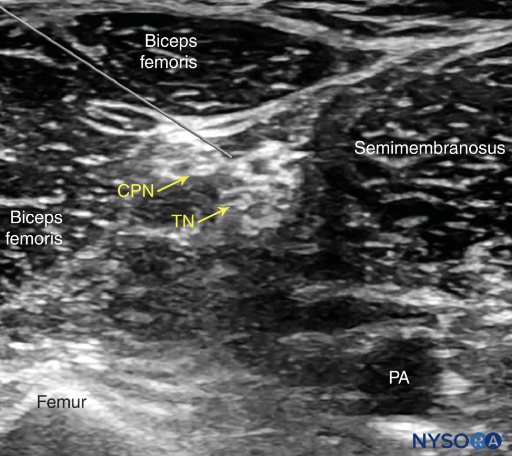
Visualizing and blocking the TN and CPN:
How do you know you’re in the right place?
The anesthetic spreads proximally and distally to the site of the injection around both divisions of the nerve, or the spread of the local anesthetic within the sheath proximal to the site of injection.
A single injection of local anesthetic typically suffices, typically 15-30cc of 0.5% ropivicaine.
Back to the case:
This patient’s anatomy was not as clear as the above example images, but below are the clips from this case.
The sciatic nerve at the split into the CPN and TN is seen just above and slightly to the right of the popliteal vessels
The patient’s pain was controlled adequately in the ER with successful reduction and splinting of the ankle fracture without any additional pain medications. The patient returned a week later, at which time she had a scheduled ORIF of her bilateral malleolar fractures with the orthopedic surgeon.
Happy scanning!
References: