
“Help, I’ve Fallen and I Can’t Get Up”
Written by: Dr. Zach Ravnitsky
Edited by: Dr. Joann Hsu
A clinical case in which we utilized Ultrasound to control the pain of an elderly woman who fell and broke her hip.
Lets begin with a case:
An 81-year-old female with a fall at home resulting in severe left hip pain and inability to bear weight, found to have an intertrochanteric femur fracture.
Tripped over a carpet while walking to the bathroom at night, landing directly on her left side
Immediate severe hip pain internally rotated Left hip
EMS gave 50 mcg fentanyl en route
The X-Ray of the left hip:

The above X-ray portrays a left intertrochanteric femur fracture. OUCH!!!
Next Steps:
Order preoperative labs
Discuss goals of care with patient and her family
Consult orthopedic surgery
Control her pain!
How can we best control this poor patient's pain?
NSAIDS
Tylenol
Muscle relaxers (methocarbamol, baclofen, tizanidine)
Lidocaine patches
Opiates
Nerve blocks
Multiple studies have shown that to control acute pain, we should do a few things, including multimodal pain medication therapy, and incorporate nerve blocks to decrease overall opiate usage and post operative delirium, especially in the elderly community.
Today we will discuss 3 relevant hip blocks, the relevant anatomy, materials needed for success, and safeguards to ensure a safe and effective nerve block.
3 Hip Blocks:
PENG (Pericapsular Nerve Group) block
IIFI (Infrainguinal Fascia Iliaca) block
SIFI (Suprainguinal Fascia Iliaca) block
To understand these 3 hip blocks we must first know the relevant anatomy, and the indications for each.
The majority of the sensory input to the hip and lower extremity is controlled by the 3 nerves below:

All of these nerves originate from the lumbar plexus.
The femoral nerve and the obturator nerve are contained within the fascia iliaca, a fascial sheath that encases these nerves and the iliopsoas muscle, as it courses distally down the leg.
The lateral femoral cutaneous nerve pierces through the iliopsoas, but does not directly course inside the fascia iliaca.
However, when doing the following nerve blocks, sometimes it will cover proximal portions of the lateral femoral cutaneous nerve as well.
PENG vs FASCIA ILIACA (IIFI and SIFI)
PENG: ***PERICAPSULAR*** nerve group block
Plane block of the articular branches of obturator, femoral, and accessory obturator nerves that sit in the fascial plane between the psoas muscle and the superior pubic ramus
best for more proximal hip fractures compared to the fascia iliaca block. For example: pubic rami, acetabular, femoral neck, and IT fractures.
Fascia Iliaca:
Plane block of femoral nn, obturator nn, lateral femoral cutaneous nn that sit within the fascia iliaca, which courses between the femoral artery and nerve at the level of the femoral head. The fascia iliaca sits on top of the iliacus muscle.
A more distal hip block compared to the PENG. It can block most of the femur (much more than the proximal femur coverage of the PENG).
SETUP:
MATERIALS:

Now lets review the 3 Blocks:
PENG:

To Identify the correct anatomy for the PENG block, you should first rest your linear transducer in the orientation as seen in line A.
You will see a hyperechoic arch, which represents the femoral head.
This should tell you to move superior towards position B. Notice in the photo on the left, line B passes over a ridge, indicated as the AIIS.
You will also see the IPE and femoral artery in view.
Your goal is to deposit your anesthetic below the PT (psoas tendon.)
If you see the PT lift off the pubic bone, you are in the right place.
It will bathe the nerves that we discussed before and relieve pain at the level of the femoral head or neck.
This benefit of this block is that it is generally safe, as you have a bony backstop to provide tactile feedback before injecting your local anesthetic.
The only downside to doing the PENG, is that it may not relieve symptoms in your patients with intertrochanteric fractures or any other fracture more distal.
InfraInguinal Fascia Iliaca (IIFI):

My personal approach to identifying landmarks for the IIFA block is to first find my landmarks that we are very familiar with to do a femoral central line (femoral vein.)
We also know the femoral vein, artery, and nerve run right next to each other.
We commonly remember the acronym “VAN” to recall the orientation of the vein being most medial, then the artery, then the nerve most laterally.
Once you move your probe laterally and successfully identify the femoral artery and nerve, you should look for a few more important structures.
In the middle of your screen you will see a big bulky round muscle, covered in a hyperechoic sheath.
This is the Iliacus muscle covered in the fascia Iliaca.
You will also notice a “pointy” muscle in the lateral aspect of your screen, which is the sartorius.
If you can identify these structures in 1 single view, you are right on track to a successful IIFI block.
You should direct your needle from lateral to medial, through the “pointy” sartorius , and through the hyperechoic fascia iliaca.
Once you pop through this sheath, you should inject a small amount of local anesthetic or sterile saline.
If you see an “unzipping” of the fascial layers, you are most likely in the right place and can direct the rest of your local anesthetic into this area.
Beware, if you see the injected fluid in a different orientation, you should take a second and consider you may be intramuscular or above the fascial sheath, and should maybe redirect your needle.
Recall, this block is great for any fracture below the femoral neck, just like our patient who had an intertrochanteric femur fracture.
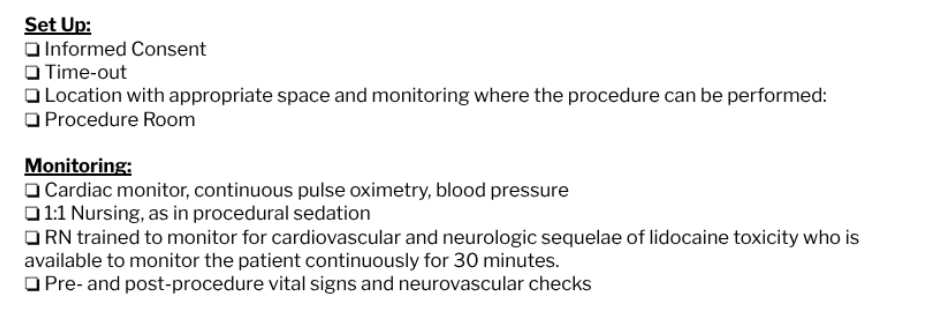
SupraInguinal Fascia Iliaca (SIFI):
The indications for SIFI are the same as the IIFI, but there is evidence that there is improved pain control in SIFI compared to IIFI if done correctly. It is slightly less safe, as there is the theoretical risk of injury to the deep circumflex iliac artery. However I hope that after this lesson, you can perform the SIFI safely and effectively.
First orient your probe in a sagittal plane just medial to the ASIS.
You should look for a bony structure in the shope of a triangle deep the musculature.
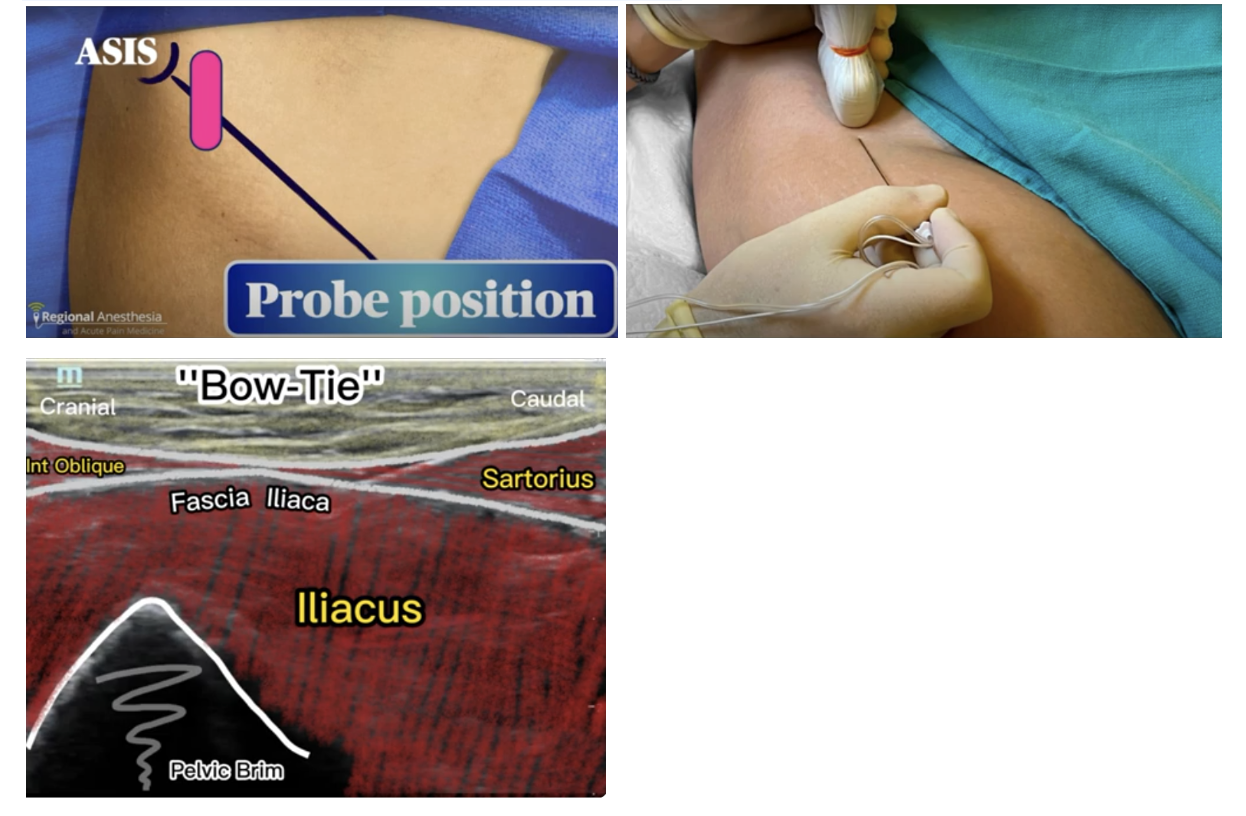
This is the pelvic rim. If you center this into your field of view, you will notice there is almost a “bow-tie” shape ( I agree, you have to use your imagination a little bit for this one.)
You will also see some familiar landmarks that you used for your other blocks.
Remember your big bulky Iliacus muscle covered in the fascia Iliaca? It is back, and you'll see it overlying the pelvic brim as seem above.
You'll also notice a “pointy” muscle, the sartorius overlying your Iliacus caudally, and your internal oblique cranially.
I hope this all makes sense (as the internal oblique is a well known portion of your abdominal wall, thus more cranial to the pelvic brim; also the sartorius is a superficial muscle of the anterior/medial thigh, so it will appear more caudal. Your goal once again is to pierce the fascia iliaca, inject your local anesthetic and “unzip the fascia.”
Beware, you must point your needle caudal to the cranial, and expect a traversing perpendicular deep circumflex iliac artery as you move more cranial.
We do not start cranially as it is more difficult to safely identify this artery.
THANK YOU! I hope you can use this guide to incorporate ultrasound into your practice and best serve your patients suffering from hip fractures!
Happy scanning!
References:
Kumar K, Pandey RK, Bhalla AP, Kashyap L, Garg R, Darlong V, Malhotra R, Yadav CS. Comparison of conventional infrainguinal versus modified proximal suprainguinal approach of fascia iliaca compartment block for postoperative analgesia in total hip arthroplasty: a prospective randomized study. Acta Anaesthesiol Belg. 2015;66(3):95-100. doi:10.2174/1874434601506030095. PMID: 26767235.
Hi X, Zhang Y, Li Z, et al. Preemptive continuous fascia iliaca compartment block reduces postoperative delirium in elderly patients with hip fracture: a randomized trial. Medicine (Baltimore). 2019;98(16):e14767. doi:10.1097/MD.0000000000014767. PMID: 31522217.
Thompson J, Long M, Rogers E, et al. Fascia iliaca block decreases hip fracture postoperative opioid consumption: a prospective randomized controlled trial. J Orthop Trauma. 2020;34(1):49-54. doi:10.1097/BOT.0000000000001634. PMID: 31469752.
Carr M. PENG (PEricapsular Nerve Group) block: A novel motor-sparing single-injection option for pelvis and hip fractures. Highland EM Ultrasound. Accessed November 23, 2025.
Kwaktalk. Fascia Iliaca Block. Block Talk. December 27, 2022. Accessed November 23, 2025. https://kwaktalk.org/block-talk/2022/12/27/fascia-iliaca-block
Nagdev A. Infrainguinal Fascia Iliaca Plane Block (AKA: Femoral Nerve Block) — Highland EM Ultrasound Fueled Pain Management. Highland Ultrasound. Published 2012. Accessed November 23, 2025.
“Supra Inguinal Fascia-Iliaca Block (SIFI Block).” YouTube, uploaded by hoCUS poCUS, 29 Jan. 2023, https://www.youtube.com/watch?v=0Fu5l_Alm7c
“Ultrasound Guided Fascia Iliaca Block.” YouTube, uploaded by Dr. Alyse Volino, https://www.youtube.com/watch?v=eO3lsnAJcq8