
Torsion
Written by: Dr. Rebecca Zhang
Edited by: Dr. Joann Hsu
Case Presentation: 78 y/o M presents to ED with testicular pain. s/p L inguinal hernia repair here 3 days ago, pain started at 4am today. No dysuria, hematuria, fever, chills, nausea, vomiting.
Physical Exam: Bilateral swelling, erythema and tenderness of the left testicle. No crepitus.
How to perform a point of care testicular ultrasound:
Step 1: Obtain two towels for privacy and view optimization
Step 2: Place towel one over penis, another under testicles, to drape the patient and only expose the area of interest
Step 3: Select linear probe - ensure that your ultrasound is on testicle setting!
Why does the setting matter?
The various presets on your ultrasound machine for different types of studies focuses on optimizing your image for the type of study you are doing.
However, some of these presets use a higher thermal index, and the testicles are sensitive to temperate increases
The testicle setting (or ocular setting, if your machine does not have a testicle setting) will use a lower thermal index to avoid potential harm to the testicle
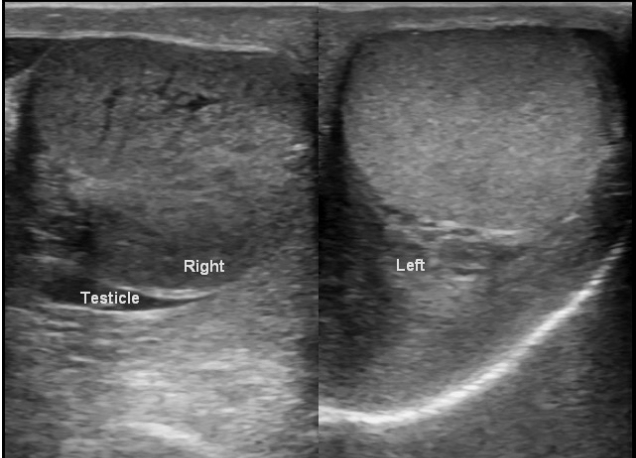
Step 4: Obtain the “buddy view “ or “owl’s eye view”
Both testicles in a transverse view to get a global look at the bilateral testicles
You can get an overall sense of symmetry and echotexture of both testicles. You can also put color doppler across the entire screen and compare the relative flows of the two testicles next to each other - does one have a lot more flow than the other? Does one have absent flow compared to the other?
Step 5: Then obtain views in sagittal and transverse of both testicles followed by color doppler of both individually, on same setting
We see the following…
Unaffected right testicle with a hydrocele
Left testicle with this finding within the scrotal sac
Left testicle with hydrocele and abnormal heterogenous appearing echotexture
In our POCUS images:
The right testicle has a hydrocele around it but the echotexture is normal.
Not shown - right testicle had both arterial and venous flow.
The left testicle has a hyperechoic mass within the scrotal sac, a heterogenous appearing left testicle, and a hydrocele.
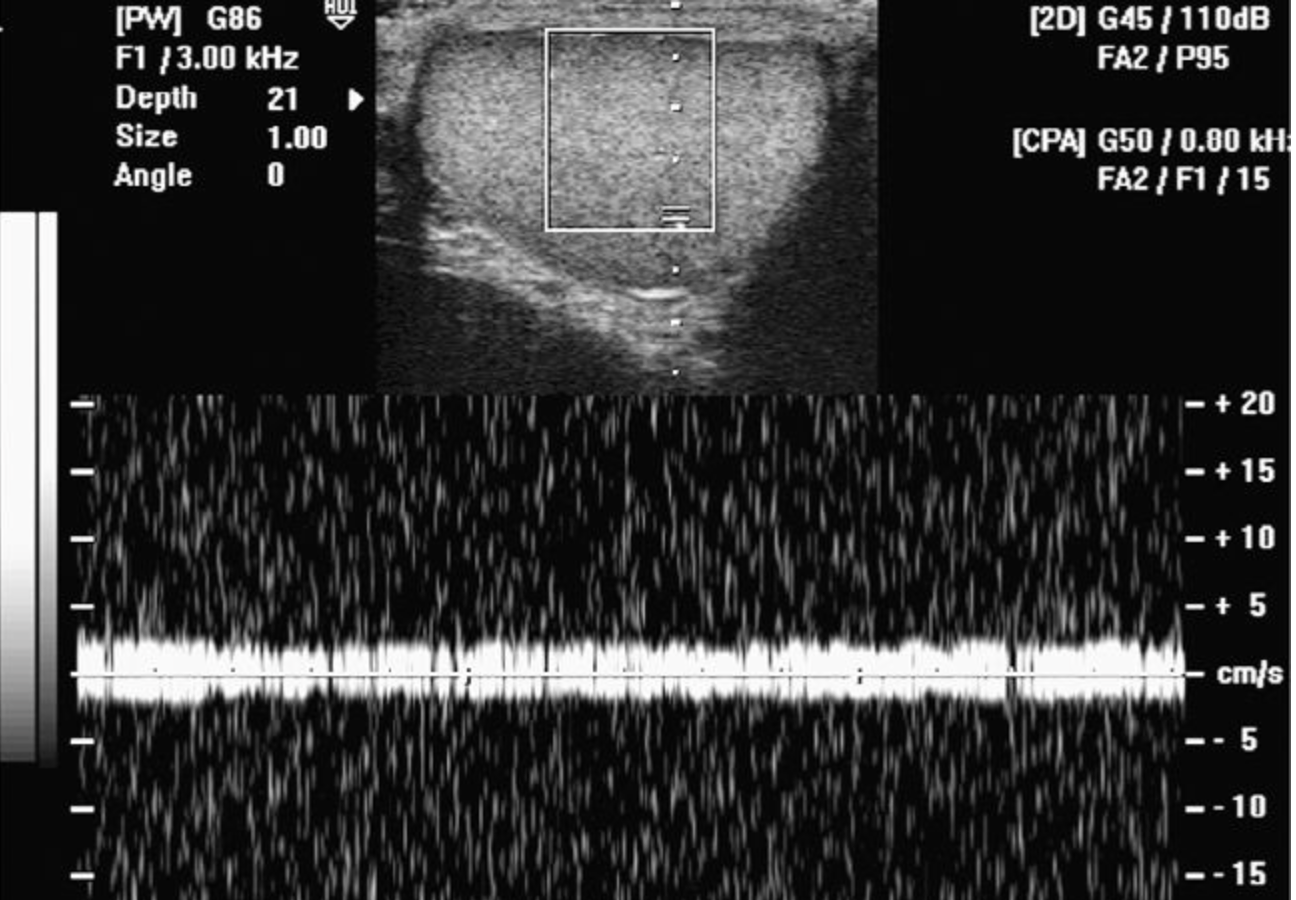
There was no blood flow noted (both venous and arterial) to the left testicle. Pictured above is color doppler on the left testicle showing significantly decreased flow compared to the right.
Let’s talk about Testicular Torsion!
Definition: Acute scrotal pain in 0-1 years old and at puberty in bimodal incidence, caused by testicular ischemia when it does not receive blood flow - usually from twisting of the spermatic cord but can also occur from extrinsic compression of the vessels
Risk Factors: Exercise, trauma, undescended testicles, bell-clapper deformity
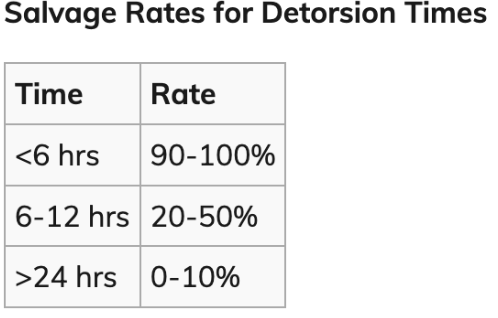
Time is Testicle! How long do we have?
What to expect on history and physical?
Abrupt onset testicular pain with nausea, vomiting.
Always ask about testicular pain in men with unilateral lower quandrant pain!
On physical exam you may see a high riding testicle with no cremasteric reflex.
Normal testicle
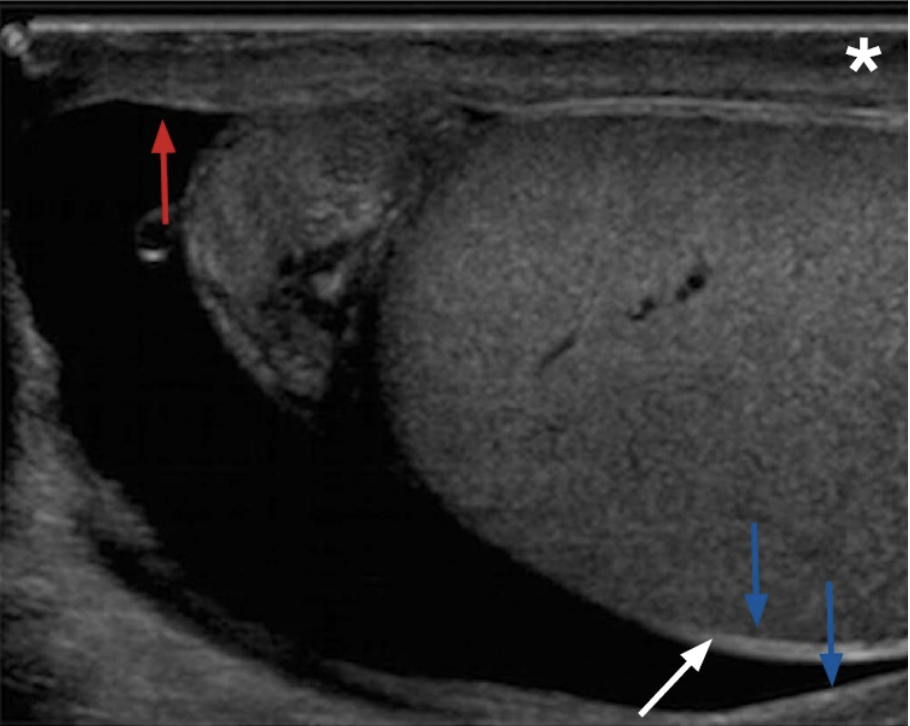
What are key features of torsion on ultrasound?
The primary feature is the absence of BOTH venous and arterial flow in the testicle using pulse wave doppler
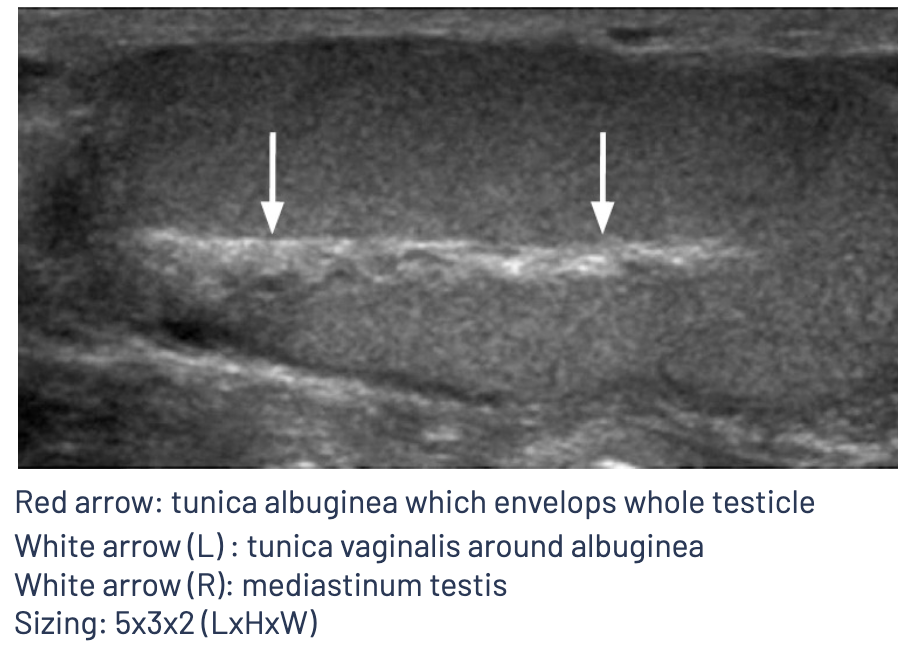
Sonographic findings of the testicle itself can be variable depending on the duration of torsion and extent of vascular compromise.
The testicle can appear enlarged and hypoechoic and the parenchyma of the testicle will become less homogenous when compared with the unaffected testicle. When the testicle becomes necrotic, the testicle can appear more heterogenous in echotexture compared to a normal testicle
Other sonographic findings include: Twisted spermatic cord (Whirlpool sign), reactive hydrocele, and thickening of the scrotal wall.
Right side torsed testicle with changes in echo-texture
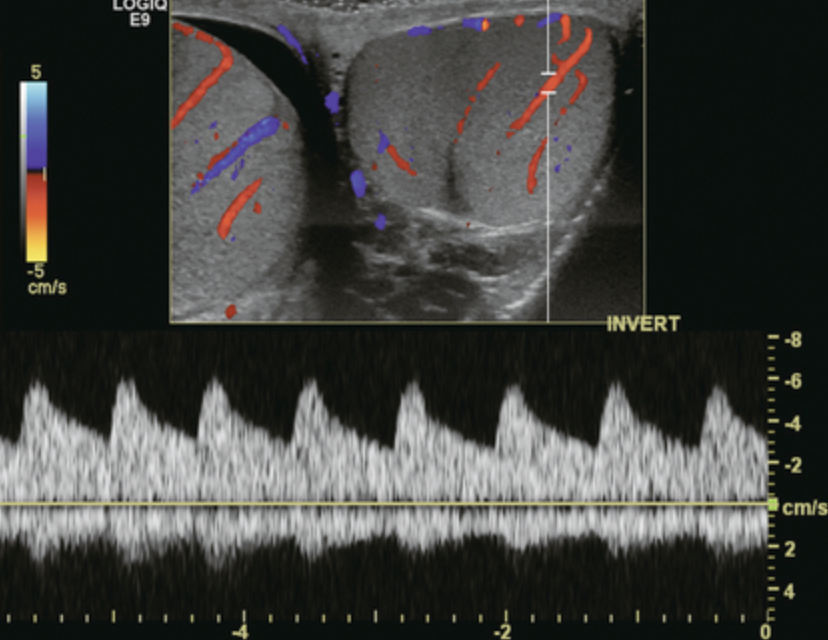
Normal low resistance arterial flow in a testicle. A normal resistive index is 0.5 - 0.7. Greater than 0.7 is concerning for early or partial torsion, as there is increased resistance in blood flow.
Salvage Maneuvers:
Consult urology, attempt manual detorsion by opening the book.
Twist 180 degrees in medial or lateral directions, up to 540 degrees.
Back to the case
The patient was sent for comprehensive scrotal ultrasound and CTAP.
He was found to have a scrotal hematoma on the left with no blood flow to the left testicle
Take Home Points: Obtain good history and physicals! Diagnostic accuracy of POCUS for testicular torsion when performed by the emergency physician is found to be 95% sensitive and 94% specific! Time is testicle!
Happy scanning!
Reference
https://radiologykey.com/testicular/
https://www.acep.org/sonoguide/advanced/testicular