
Right heart strain on POCUS
Written by Dr. Dan Ng
Edited by: Dr. Joann Hsu
Case:
71 year old female presented with complaint of fatigue, generalized weakness and nausea. Patient was found to be hypoxic to 91% on RA. States she has this generalized feeling of weakness. However denies fever, chills, chest pain, SOB, abdominal pain, diarrhea or dysuria. Has not had any hematuria, hematochezia, melena, or vaginal bleeding. Denies sick contacts. Does not use any oxygen support at home.
Vitals:
82 BPM • 106/75 • RR 18 • 91% RA • Afebrile
Focused exam:
Other than 91% on RA, unremarkable Gen, skin, ENT, cardiac, respiratory, abdomen, extremity, neuro exam.
The patient is presenting with very vague complaints with a nonfocal exam.
However, you notice that the patient is objectively hypoxic, so you grab the ultrasound.
Lung ultrasound is unremarkable, but the bedside echo shows:
Six signs of right heart strain on POCUS
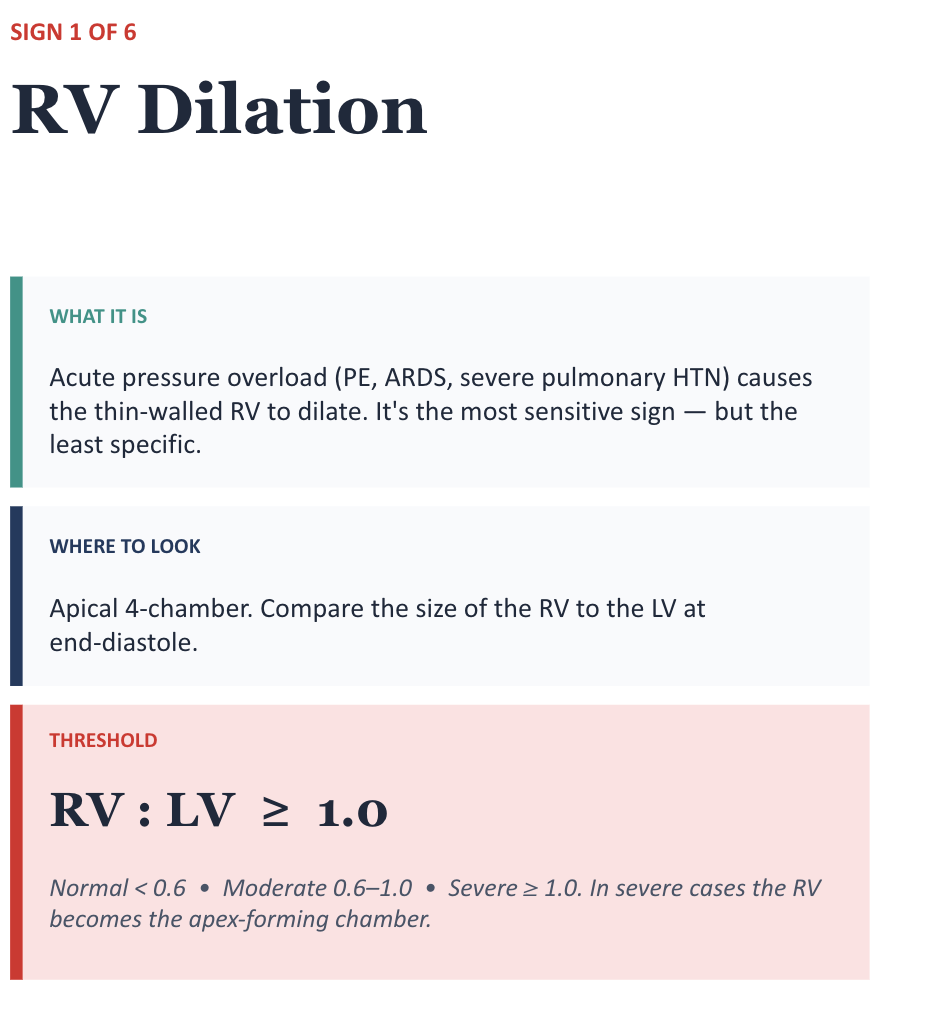
RV dilation (RV:LV ratio > 1)
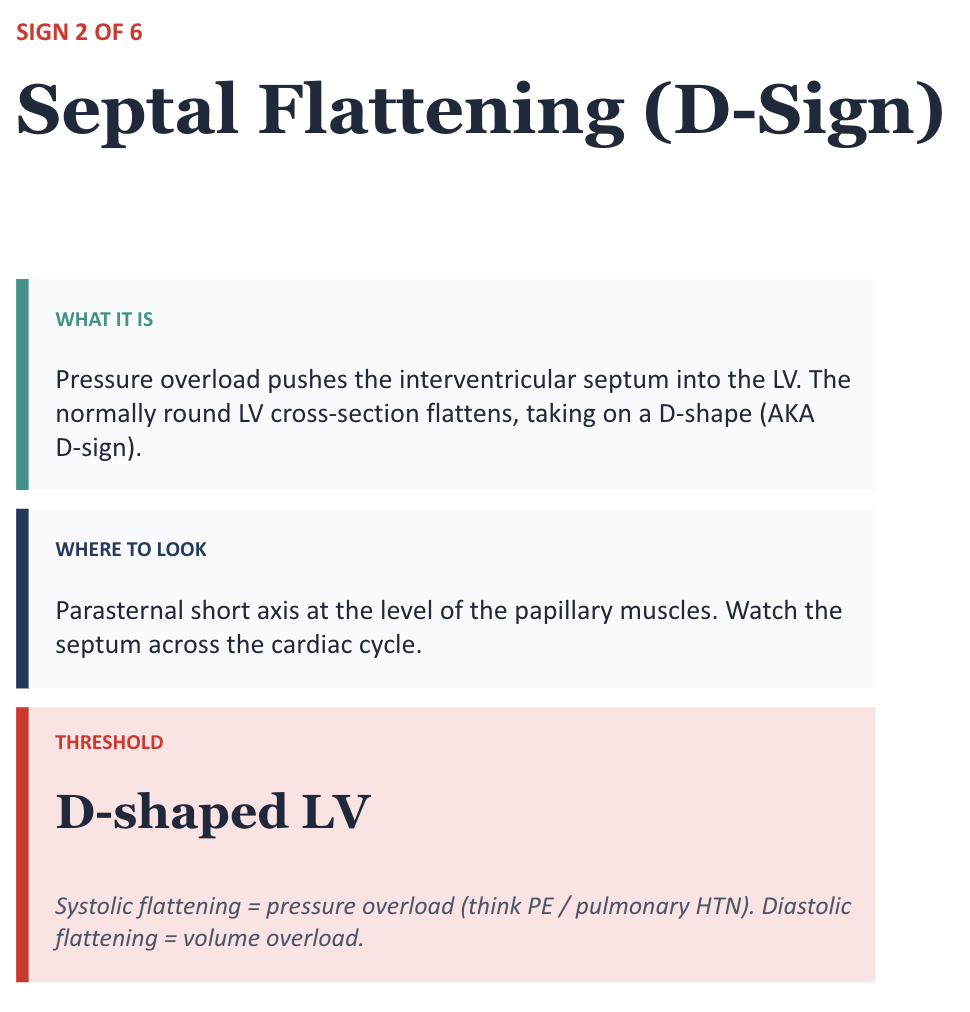
Septal flattening aka D SIGN
McConnell’s sign: akinesis of the RV walls with apical sparing
TAPSE <17 mm indicates right heart strain
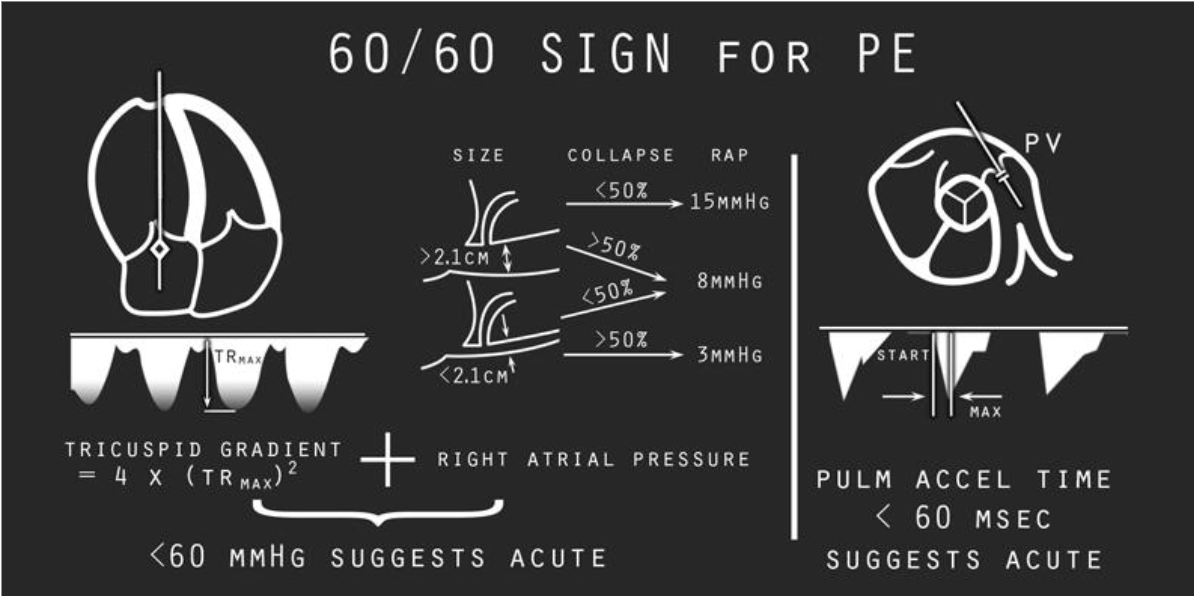
60/60 sign: increases specificity for ACUTE right heart strain
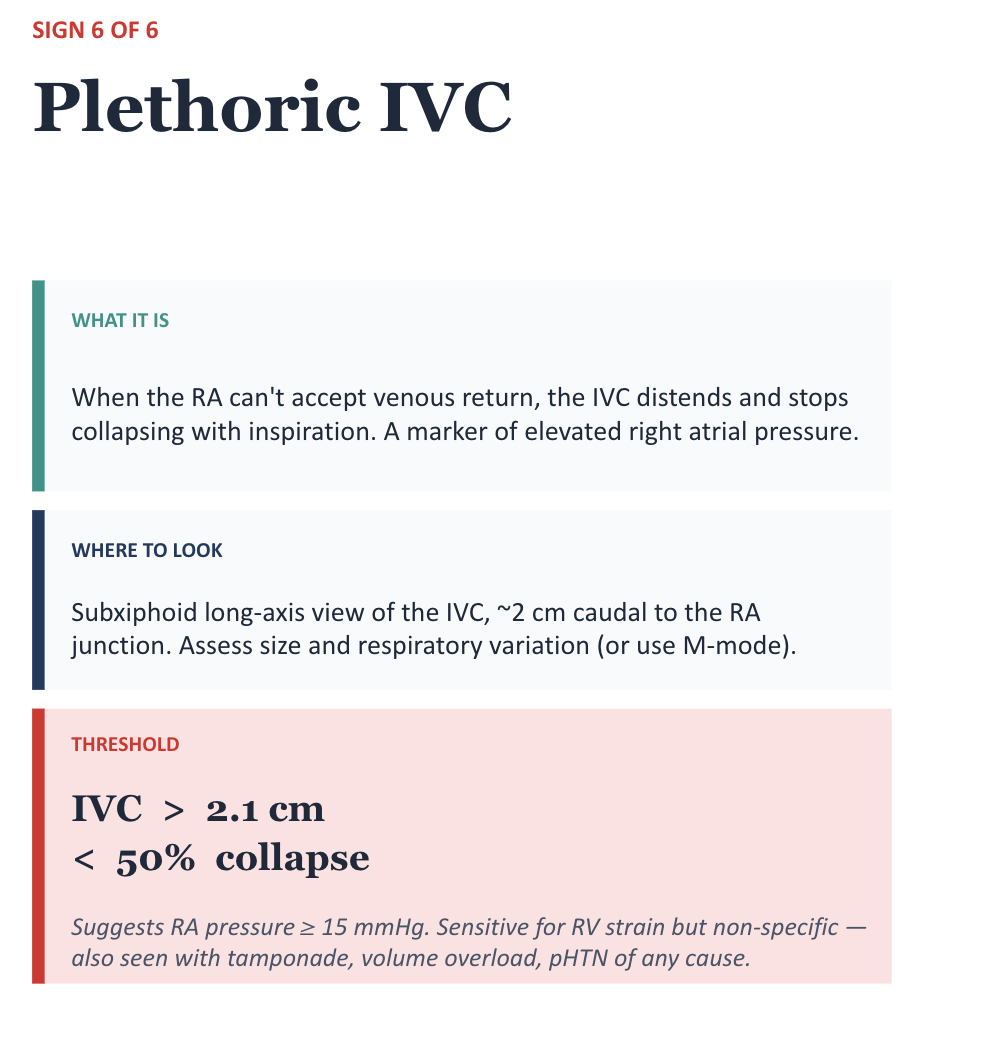
Plethoric IVC: >2.1 cm with no respiratory variation



It looks like the RV apex is the only thing contracting in the RV. This case is an excellent example of McConnell’s sign.
McConnell’s sign has a low sensitivity and high specificity for acute PE but there is a pretty wide range.
McConnell’s sign is NOT pathognomonic for acute PE!! Chronic conditions can also have this.
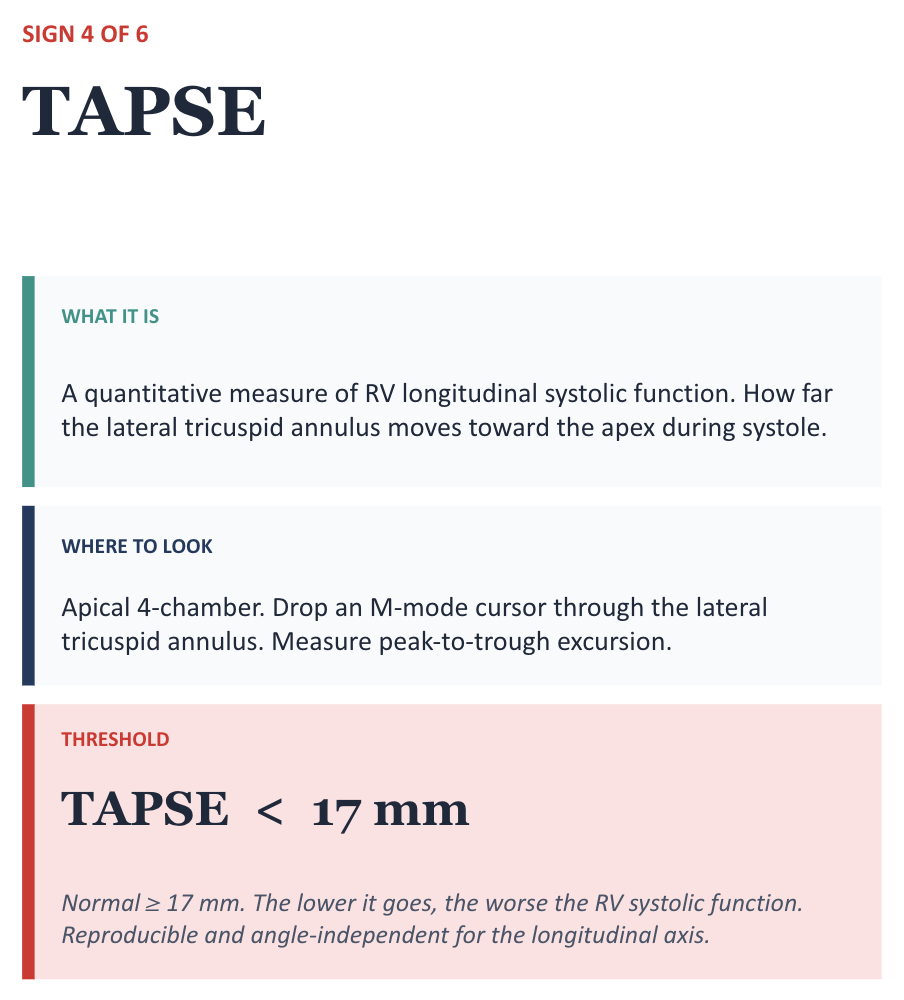
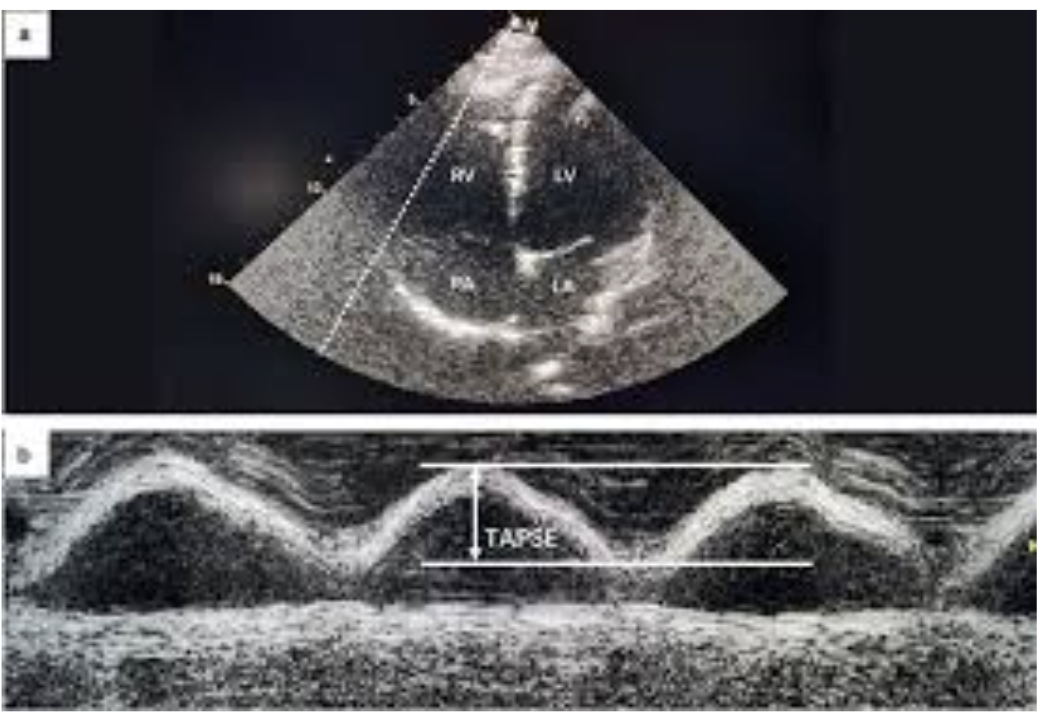
This basically measures if there is a decrease in movement of the RV at the tricuspid annulus which occurs as right heart strain worsens. The less movement there is, the more concerning. Therefore, an abnormal TAPSE is one that is LESS than 17 mm.

CLINICAL PEARL Highly specific for acute PE when present. Negative doesn't rule it out; it's a rule-in tool.

Case resolution:
CT Chest showed: Extensive saddle embolism involving both lungs with evidence of right heart strain. Persistent posterior basal right lower lobe 2.7 cm nodular consolidation.
Patient admitted to MICU
Patient was continued on alteplase at 1 mg/hr for 20 hours as well as heparin drip. TTE was done and showed RV severely dilated. Reduced RV systolic function. Mild to moderate TR. US doppler of lower extremities showed acute DVT in the L popliteal and posterior tibial veins
Patient was downgraded to the floor and continued to do well. Heparin drip was transitioned to PO Apixaban.
Take home points:
Six signs, one question: is the RV in trouble?
RV dilation, D-sign, McConnell's, TAPSE, 60/60, plethoric IVC.
Sensitive signs cast the net; specific signs rule in acute strain.
Remember that many of these signs are NOT specific for ACUTE right heart strain and can be seen in chronic right heart strain conditions, like pulmonary hypertension.
60/60 sign attempts to increase the specificity for acute PE, but has poor sensitivity
McConnell’s sign has higher specificity for acute PE but poorer sensitivity
Good idea to POCUS your hypoxic patients
More signs = higher pre-test probability. Don't hang your hat on one finding. CLINICAL CONTEXT MATTERS!
Happy scanning!