
Out of Bounds: Meckel's Diverticulum Past it's Age Limit
Written by: Dr. Michelle Qu
Edited by: Dr. Joann Hsu
Case Presentation
35 year old male with a past medical history of HTN presents to the ED for right lower quadrant abdominal pain for 12 hours. Around 8-9 PM, he had central abdominal pain and right lower quadrant abdominal pain that progressed to subjective fever and chills.
Initial Vitals
BP: 113/63
Pulse: 92
Resp: 18
Temp: 37.7 °C
SpO2: 93%
Physical Examination:
CHEST AND RESPIRATORY: (-) rales, (-) rhonchi, (-) wheezes; breath sounds equal bilaterally.
HEART AND CARDIOVASCULAR: (+) tachycardia to 120s BPM; normotensive; (-) murmur, (-) gallop.
ABDOMEN AND GI: Soft; (+) right lower quadrant tenderness, (-) psoas sign, (-) obturator sign, (-) guarding, (-) rebound, (+) mild distension.
RLQ US:
Remainder of the ED course
Appendcitis was high on the differential with what looked like an appendocolith in the right lower quadrant with posterior acoustic shadowing. CT was ordered which showed the following:
CT impression :
Right lower quadrant mid ileum 5.4 x 3.5 x 3.3 cm diverticulum, which may represent Meckel's diverticulum, containing calcifications/stones. Surrounding inflammatory fat infiltration suggesting Meckel's diverticulitis. Proximal small bowel distention with air-fluid levels, which may represent ileus versus partial small bowel obstruction. Unremarkable appearing appendix.
Surgery was consulted. Patient was admitted under surgery for planned for diagnostic laparotomy, possible exploratory laparotomy, possible diverticulectomy, possible small bowel resection.
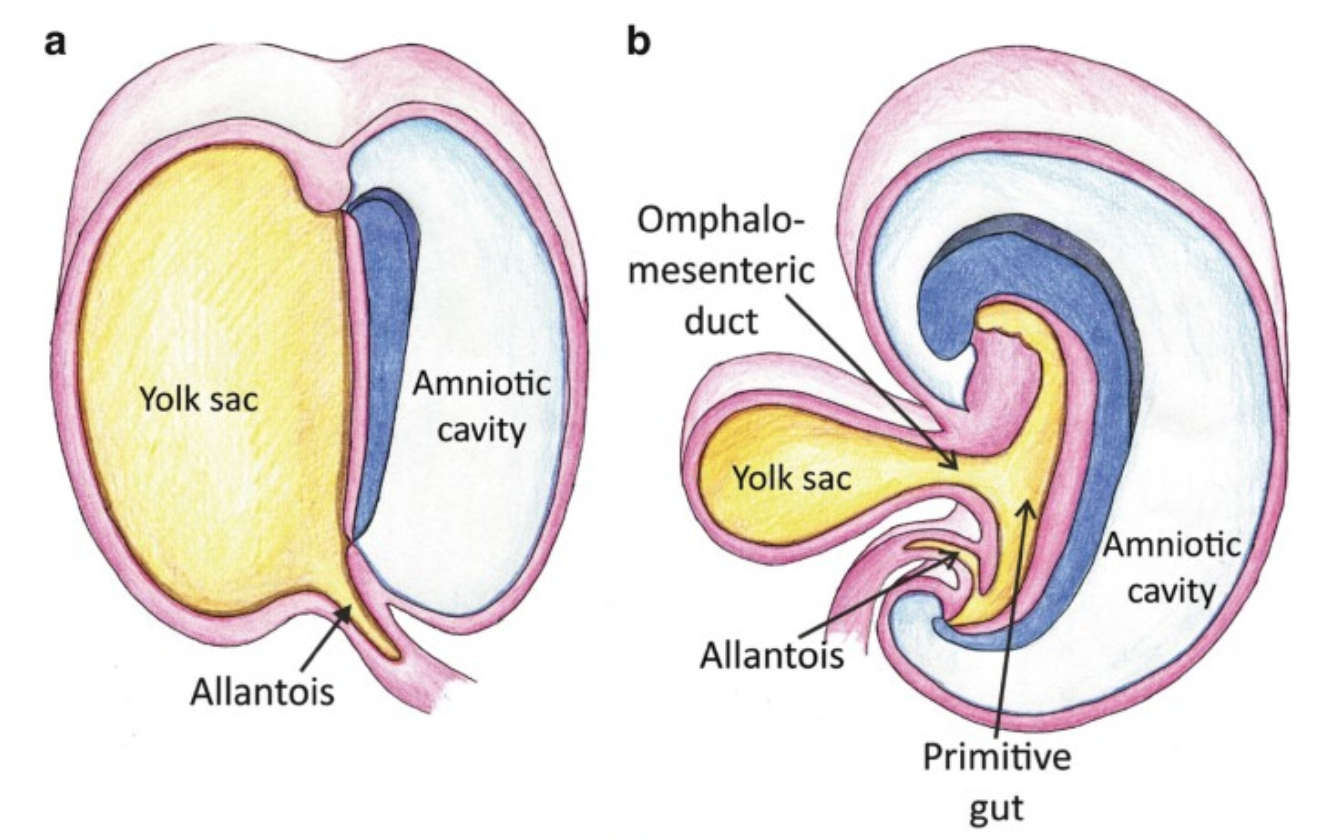
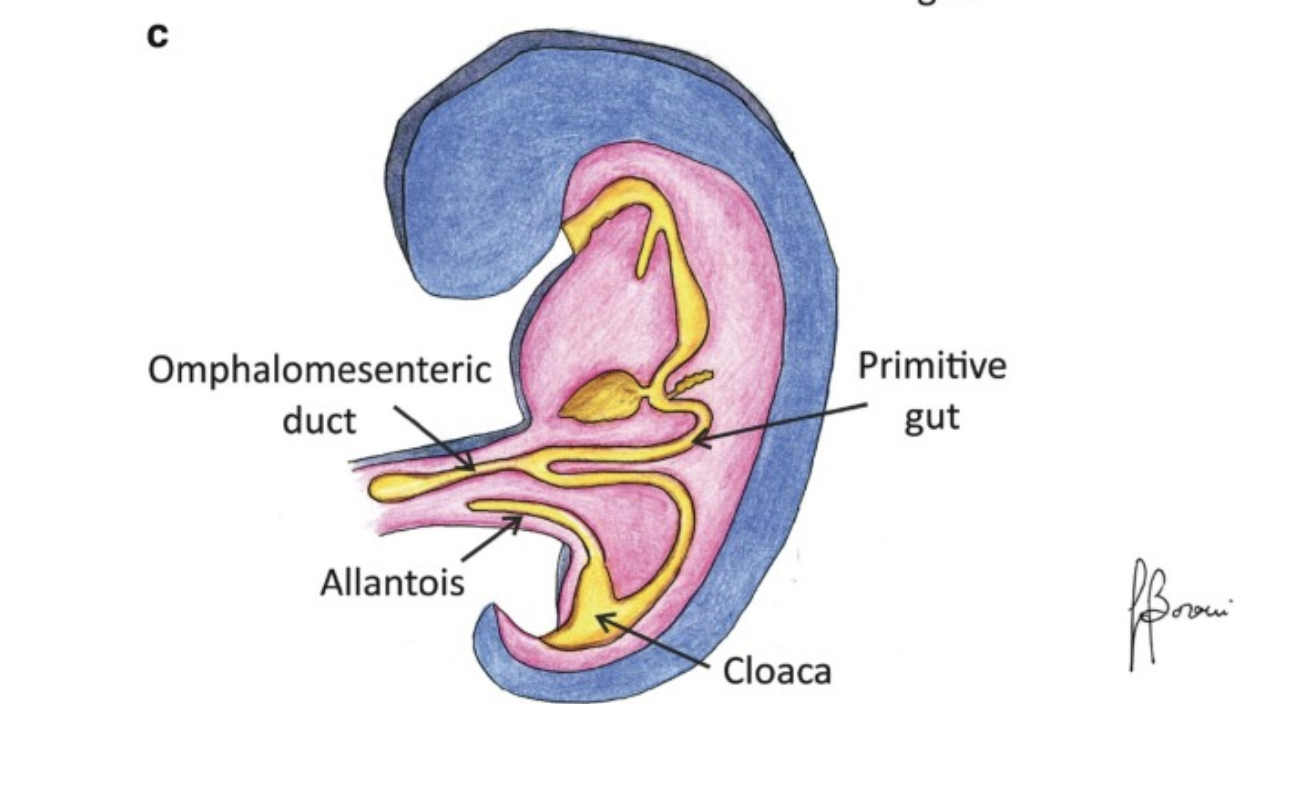
Meckel’s Diverticulum
Mecke’s diverticulum is the remnant of the omphalomesenteric duct, found at the antimesenteric border of the terminal ileum.
Typically, the diverticulum about 3cm proximal to the ileocecal valve.
It is the most common congenital anomaly of the gastroinetsintal tract, occurring in 1-3% of the general population.
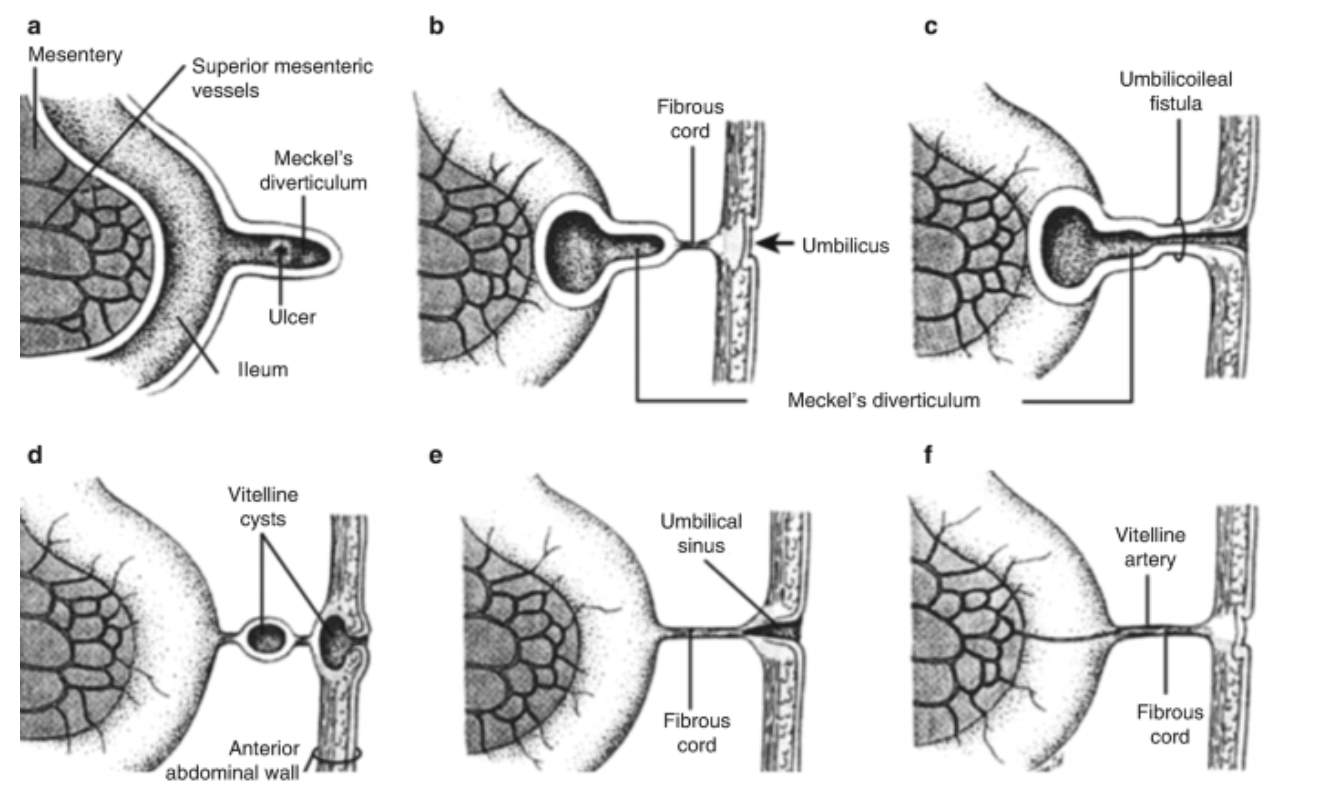
Major complications include bleeding, obstruction, intussusception, diverticulitis and perforation. Bleeding occurs in the diverticulum because it can contain gastric mucosa that secretes hydrochloric acid which causes ulcerations leading to bleeding.
Clinical presentations differ by age.
In children, the most common presentation is lower GI bleeding (52%) followed by obstruction (29%), umbilical problems (10%) and diverticulitis (8%).
In adults, the most common presentaiton is diverticulitis (47%) followed by obstruction (30%), GI bleeding (20%) and umbilical problems (3%)
Rules of 2s
Meckel’s diverticulum is predominantly a disease of the young. Typically is taught in medical school as the “rule of 2s.'“
2% prevalence in the general population
Presents in the first 2 years of life (in symptomatic cases
Located approximately 2 feet from the ileocecal valve
Approximately 2 inches in length
2 types of ectopic tissue (gastric and pancreatic)
2:1 male to female ratio in symptomatic cases
However, the rules of 2 do not always apply.
While more than 50% of bleeding cases present by age 2 years, overall 60% of all symptomatic patients present before age 10 years old and 50% before age 20 years old.
Therefore, many cases present well beyond 2 years of age.
This patient presented at 35 years old. The distance is actually closer to 20 inches from the ileocecal valve rather than 2 feet.
It is more predominant in males, however, the rules of 2s underestimates this predominance. It is usually up to 4x more common in males.
Risk Factors
Four features are most commonly asociated with symptomatic Meckel’s diverticulum:
Age younger than 50 years old
Male sex
Diverticulum length greater than 2 cm
The presence of histologicaly abnormal tissue or inflammation.
This patient had all of the risk factors above. While it can’t be determined if this patient had ectopic tissue in the ED setting, there were definitely CT findings suggesting inflammation in the area.
Diagnostic modalities
Technetium-99m pertechnetate (Meckel) scan - Study of choice for detecting ectopic gastric mucosa.
The sensitivity is 85-92% in children but only 62-88% in adults. Overall specificity is 95% and accuracy 90%
Other diagnostic modalities include small bowel capsule endoscopy (SBCE), Device-assisted enteroscopy which has a high sensitivity but is an invasive procedure, and CT enterography which is often nonspecific unless there is associated inflammation or intussusception.
Multimodality approach is often required for diagnosis
Management
Meckel’s diverticulum is definitively treated by surgical resection, either open or laparoscopic approaches are safe and effective.
Surgical options include simple diverticulectomy (19% incidence) or partial small bowel resection (81% incidence), depending on the complications involved.
Utilizing Ultrasound in Diagnosing Meckel’s Diverculitis
Ultrasound has a higher accuracy in pediatric patients than adults in diagnosting Meckel’s diverticuliits, similarly in the setting of appendicitis.
In a large study involving 784 children, ultrasound demonstrated a sensitivity of 93.6% and a specificity of 98.1%.
The characteristic features of inflamed Meckel’s diverticulum can include the following findings:
Fixed, blind ending tubular or cystic structure in the bowels.
Thickened wall
Irregular mucosal layer
Tubular hyperechoic structure
Surrounding hyperechoic fat representing pericolic inflammation
May contain fluid, air or particulate material
Hyperemia in the diverticular wall indicating inflammation
Increased vascularity in the surrounding hyperechoic layer, which suggests perforation
Small bowel obstruction may be present as a complication
However, many of the above findings in the right lower quadrant can be mistaken for other conditions such as appendicitis and intussusception in the right age group.
There are limitations in ultrasound use in adults as most of the published data involves the pediatric populations.
Happy scanning!
References:
https://pubmed.ncbi.nlm.nih.gov/30170459
https://pubmed.ncbi.nlm.nih.gov/40906021
https://pubmed.ncbi.nlm.nih.gov/10706156
https://pubmed.ncbi.nlm.nih.gov/24948825
https://pubmed.ncbi.nlm.nih.gov/40072474
https://pubmed.ncbi.nlm.nih.gov/38857483
https://pubmed.ncbi.nlm.nih.gov/41046305
https://pubmed.ncbi.nlm.nih.gov/15729078
https://pubmed.ncbi.nlm.nih.gov/32224041
https://pubmed.ncbi.nlm.nih.gov/32076751
https://pubmed.ncbi.nlm.nih.gov/12540446
https://pubmed.ncbi.nlm.nih.gov/15244309
https://pubmed.ncbi.nlm.nih.gov/40696289
https://pubmed.ncbi.nlm.nih.gov/40874366