
The Gassy Gallbladder
The Gassy Gallbladder: Role of POCUS in Emphysematous Cholecystitis
Written by: Jing Jing Gong, MD. Edited by: Jeff Greco, MD
Overview:
Emphysematous cholecystitis (EC) is a rare but deadly variant of acute cholecystitis (AC). Although EC comprises of only 1% of all cases of AC, it is associated with higher mortality compared to AC and is deemed a surgical emergency. Emphysematous cholecystitis has a rapid, insidious onset, and is pathologically due to ischemia of gallbladder and infection of gallbladder wall secondary to gas-producing organisms including Clostridium, E coli, Klebsiella, and B fragilis. This condition places patients at increased risk of gangrene and perforation of gallbladder. While the “gold standard” diagnostic modality of this condition is computed tomography (CT) for its high sensitivity and specificity, point-of-care bedside ultrasonography (POCUS) has become a common modality in ED setting for rapid imaging and for visualization of the gallbladder. Furthermore, because patients who present with EC may have different symptoms from those with AC, not all patients would receive CT imaging. Table 1 below from Safwan & Penny, 2016 lists the clinical differences between the two.

Table 1: Safwan & Penny 2016
Because sound waves do not travel as well through air as through fluid, emphysematous cholecystitis can be diagnosed on ultrasound based on reverberation artifacts when air is present in the gallbladder. Although POCUS sensitivity is lower than that of CT, POCUS for EC has a specificity of 90-95%.
Visualization:
As the patient lays supine, ultrasound operator can visualize the patient’s gallbladder with the curvilinear ultrasound probe positioned perpendicular to patient’s subcostal region and slide laterally in sagittal alignment (marker cephalad). Once the gallbladder is identified, the probe can be turned counter-clockwise by 90 degrees to better visualize the gallbladder in the perpendicular axis. Air in gallbladder can be detected in patients 72 hours after onset of symptoms.
There are 3 stages of emphysematous cholecystitis based on sonographic findings. Stage 1 is characterized by the presence of air in gallbladder lumen, seen as hyperechoic line with “dirty shadowing” (Images 1 & 2). Stage 2 is characterized by air in the gallbladder wall (Image 3). This air in wall produces a highly reflective gallbladder wall that reverberates as patient moves, and depending on the patient’s position, may produce a hyperechoic ring around the gallbladder. Stage 3 is characterized by air in the pericholecystic tissue, in the gallbladder, in the gallbladder wall, and also outside the gallbladder. This is the most severe stage, as it suggests gangrene and perforation.
While there are no specific diagnostic findings on ultrasound for gangrenous cholecystitis, there are a few features associated with the condition. Specifically, the thickened gallbladder wall may exhibit striations. In 5% of cases there may also be a visible intraluminal membrane (Image 4). Other features include asymmetry of GB wall, echogenic debris suggesting “biliary sludge” in gallbladder lumen, and pericholecystic fluid collections. Note the latter half of this list is not specific to gangrenous cholecystitis, but may also be present in acute cholecystitis when visualized with ultrasound. Interestingly, US Murphy’s sign is negative in 70% of gangrenous cholecystitis, which deviates from patients with conventional acute cholecystitis (Table 1). This difference has been suggested to be due to ischemia and denervation in gallbladder in cases of severe pathology.
The “effervescent” sign, also known as the “champagne” sign, is seen in emphysematous cholecystitis. As air bubbles form, they become multiple echogenic foci that can rise from the gravity-dependent portion of the gallbladder and dynamically “float” to the non-dependent portion of the gallbladder, similar to air which rise from the bottom of a glass of champagne (Image 5).

Image 1: Transverse view of gallbladder showing small amount of air reverberation artifact. Source: Safwan & Penny, 2016, original image by radiopaedia.

Image 2: Emphysematous cholecystitis clip demonstrating multiple echogenic foci along gallbladder wall in longitudinal view of gallbladder. Source: POCUS Atlas, by Dr. Singh
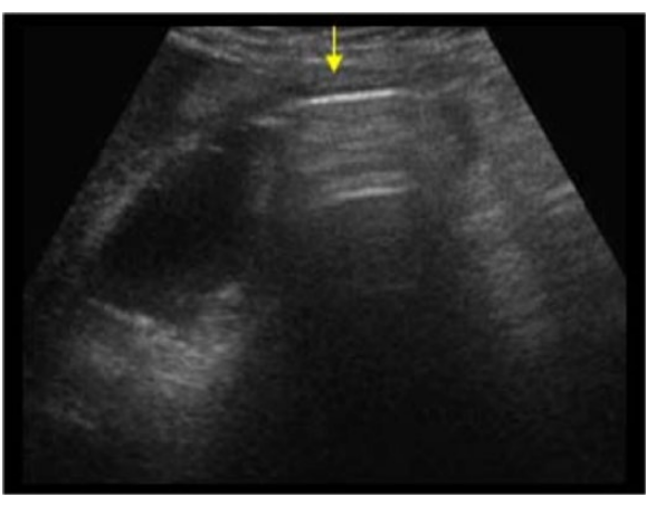
Image 3: Long view of gallbladder with hyperechoic line and a band of acoustic shadowing and reverberation in lumen due to air from emphysematous cholecystitis. Source: Safwan & Penny, 2016

Image 4: Longitudinal view of gangrenous gallbladder with visualization of intraluminal membrane (triangular arrow) and debris (white arrow). Source: Haffar 2013, Gore et al., 2010

Image 5: Longitudinal view of gallbladder demonstrating “champagne sign” seen in emphysematous cholecystitis as air bubbles of echogenic foci move from gravity-dependent regions of gallbladder toward non-dependent region. Source: Radiopaedia
Limitations:
While ultrasound has a high specificity, it is not as sensitive as CT imaging for emphysematous cholecystitis. Thus, US can rule in EC, but cannot rule out the condition.
POCUS studies are operator-dependent. Clinicians must be trained and experienced to be able to obtain high-quality ultrasound images.
Gas within gallbladder wall may be highly echogenic and difficult to distinguish from calcification of gallbladder wall, leading to inability to differentiate from porcelain gallbladder. Additional imaging modality such as X-ray to assess for radiolucency may be beneficial for differentiation.
If there is extensive gas in gallbladder, reverberations may completely obscure the gallbladder and cause US operator to interpret image as bowel and thus a false-negative study.
Adenomyomatosis is a benign condition that occurs due to hyperplasia of gallbladder mucosa. Cholesterol crystals are deposited in gallbladder wall diverticula known as Rokitansky-Aschoff sinuses, leading to visualization of hyperechoic foci with comet tail artifacts that may be mistaken for air in gallbladder. However, these cholesterol comet tail artifacts taper, unlike those of reverberations due to gas.
Conclusion:
POCUS is a fast, accessible imaging modality to evaluate patients who present with clinical symptoms of acute cholecystitis and may be under high clinical suspicion for emphysematous cholecystitis. While CT is highly sensitive, image acquisition in ED may be delayed, and US can be done during waiting time. However, for POCUS to be effective, operator must be experienced with image acquisition and recognize the limitations associated with this imaging modality.
References
Aherne A, Ozaki R, Tobey N, Secko M. Diagnosis of emphysematous cholecystitis with bedside ultrasound in a septic elderly female with no source of infection. J Emerg Trauma Shock. 2017;10(2):85-86. doi:10.4103/JETS.JETS_75_16
Baba Y, Venkatesh M. Gangrenous cholecystitis. Radiopaedia. Accessed November 11, 2020. https://radiopaedia.org/articles/gangrenous-cholecystitis?lang=us
Bloom RA, Libson E, Lebensart PD, et al. The ultrasound spectrum of emphysematous cholecystitis. J Clin Ultrasound. 1989 May. 17(4): 251-256.
Bloom, RA et al. Emphysematous cholecystitis. Medscape. Accessed November 7, 2020. https://emedicine.medscape.com/article/173885-overview#a1
Gore RM, Thakrar KH, Newmark GM, Mehta UK, Berlin JW. Gallbladder imaging. Gastroenterology Clinics of North America. 2010; 39(2): 265 – 287.
Haffar, Samir. Ultrasound of acute chronic cholecystitis. Slideshare.net, published Sept 2013. Accessed November 11, 2020. https://www.slideshare.net/shaffar75/ultrasound-of-acute-chronic-cholecystitis
Kecler-Pietrzyk, Aneta. Emphysematous cholecystitis: champagne sign. Radiopaedia. Accessed November 7, 2020. https://radiopaedia.org/cases/emphysematous-cholecystitis-champagne-sign?lang=us
Rodríguez ÁL, Pavón RF, Rionda PJ, et al. "The Effervescent Gallbladder": A Rare Ultrasonographic Finding that Reflects the Presence of Gas within the Gallbladder. Ultrasound Int Open. 2015;1(2):E72-E75. doi:10.1055/s-0035-1564155
Safwan M, Penny SM. Emphysematous cholecystitis: a deadly twist to a common disease. Journal of Diagnostic Medical Sonography. 2016 February. 32(3): 131-137.
Singh, Sukh. Cholecystitis-Emphysematous. The Pocus Atlas. Accessed November 7, 2020. https://www.thepocusatlas.com/hepatobiliary-2
Sunnapwar A, Raut AA, Nagar AM, Katre R. Emphysematous cholecystitis: Imaging findings in nine patients. Indian J Radiol Imaging. 2011;21(2):142-146. doi:10.4103/0971-3026.82300