
Distal Radius Fractures and Splinting
Written By: Richard Gallardo, MD; Edited by: Timothy Khowong, MD, MSEd

Anatomy: Where is the Radius?
The radius is the lateral bone of the forearm when standing in anatomical position. It articulates proximally with the distal humerus and articulates distally with the scaphoid and lunate carpal bones. The distal radius also forms a pivot joint with the distal ulna, allowing for supination and pronation of the forearm. Palmar and dorsal radioulnar ligaments arise from the medial border of the distal radius and insert at the styloid/fovea of the ulna, and are key for stabilizing the joint. The blood supply of the distal radius is extensive and is made up of branches of the radial artery, ulnar artery, and interosseous artery. Innervation of the distal radius is also considerable and corresponds to the innervation of the overlying skin.

Presentation of Injury
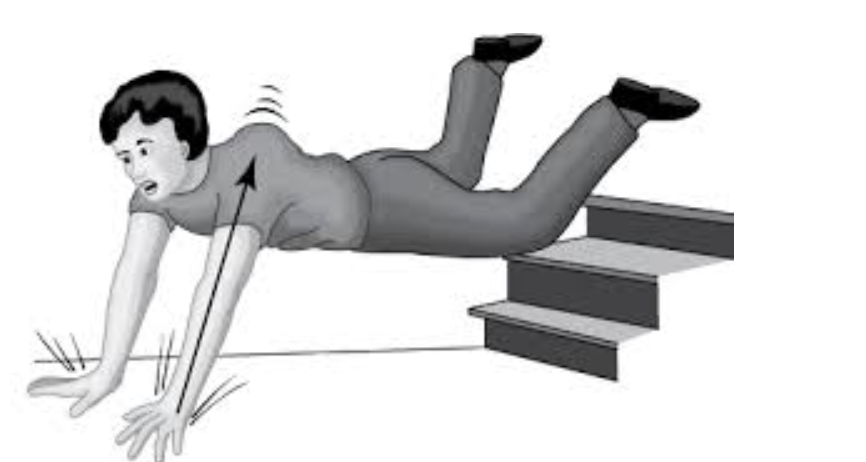
Distal radius fractures most commonly occur in a bimodal distribution, usually in children less than 18 years old and adults greater than 50 years old. The mechanism is most commonly a FOOSH injury, but can also be due to violent/high intensity injury directly to the bone. Patients with osteoporosis are especially vulnerable to distal radius fractures. Physical examination must be thorough, looking for any visible deformities, swelling, assess neurovascular status, and range of motion. It is also important to not miss any other injuries, as this may be a distracting injury.
Classification: More than one way to break a radius
Although there is no agreed upon classification system, there are multiple common ways to describe and categorize distal radius fractures. One method is to describe if the fracture is extra-articular vs intra-articular and if the fracture is non-displaced vs displaced.

One of the classification systems is called the Frykman classification system. In this classification system, there are 8 types of distal radius fractures, with the even numbers corresponding to the previous type + an ulnar styloid fracture. Types I/II are transverse metaphyseal fractures and are completely extra-articular. Types III/IV extend into the radiocarpal joint. Types V/VI are transverse fractures extending into the distal radioulnar joint. Types VII/VIII involve both the radiocarpal and radioulnar joints and are highly unstable.

Wristography

Radial Inclination
The angle between two lines drawn from the central reference point; one line drawn perpendicular to the long axis of the radius and the second line drawn to the distal tip of the radial styloid.

Radial Height
The distance between two lines drawn perpendicular to the long axis of the radius; one at the central reference point and the second line at the distal tip of the radial styloid.

Ulnar Variance
The distance between two lines drawn perpendicular to the long axis of the radius; one at the central reference point and the second line at the distal surface of the ulnar head.

Lateral View
In a normal lateral XR view of the distal radius, the radius and ulna should be superimposed. The pisiform carpal bone should also be projected over the distal pole of the scaphoid carpal bone.

Palmar Tilt
This refers to the angle created by two drawn lines; one line being perpendicular to the long axis of the radius and the second line drawn through the palmar and dorsal distal radial apices.

AP Distance
This refers to the distance between the dorsal and palmar apices of the distal radius.
The Usual Suspects
There are many different ways that the distal radius can fracture, but these are some of the most common fracture patterns.
Colles’ Fracture:
This usually results from a FOOSH injury, or high energy impact injury in younger patients. It is a fracture to the distal radial metaphysis with dorsal displacement of the distal radius fragment with no involvement of the articular surfaces.

Smith Fracture
Also results from a fall onto or direct injury to the dorsum of the wrist. It is a fracture of the distal radial metaphysis with volar displacement of the distal radial fragment. Can be further divided into 3 types. Type 1 is extra-articular and transverse (~85%). Type 2 is intra-articular and oblique, same as volar Barton’s fracture (~13%). Type 3 is a juxta-articular oblique fracture; uncommon type (<2%).

Barton Fracture (Dorsal and Volar)
Unstable intra-articular fractures of the rim of the distal radius, often associated with disruption of the radiocarpal ligament and thus, dislocation of the carpal bones. Dorsal Barton fractures often result from a fall onto a dorsiflexed/pronated wrist with the avulsed fragment migrating dorsally. Volar Barton fractures often result from a fall onto a supinated wrist with the avulsed fragment migrating volarly.

Chauffeur Fracture (aka Hutchinson)
This often results from either a FOOSH injury or a direct blow to the back of the wrist. Historically, this fracture affected drivers who would start cars using a hand crank. If there was a kickback, the crank would impact the wrist, causing it to hyper-extend and forcing the scaphoid into the radius. It is an intra-articular fracture of the radial styloid, which can vary in size.

Galeazzi Fracture-Dislocation
Similar to the other fractures, this is also a result of FOOSH injuries, although it is an uncommon injury pattern. Unlike the other fractures of the distal radius, this pattern also includes a concomitant dislocation of the distal radioulnar joint. This dislocation can be easy to miss on imaging and must be considered in any distal radius fracture. This is also divided into dorsal and volar Galeazzi fractures with the direction of the ulnar deviation determining the type.

Well what do you want me to do about it? Management in the ER
Initial Evaluation
All patients with distal radial fractures should receive medications for pain control, immobilization, and evaluation for open injury or neurovascular compromise. Before any attempt at reduction/splinting, consider any indications for an emergency Orthopedics consult: Neurovascular compromise including pulseless extremity, motor deficit, any suspicion for compartment syndrome, and any possibility of open fracture. Unstable fractures should also be referred to Orthopedics. This includes fractures that are palmarly displaced, have significant displacement or comminution, fractures with dislocations, or any fracture with injury to scaphoid (scaphoid fracture or injury to the scapholunate ligament).
Pain Control
Comparison of fracture hematoma block vs nerve block (cubital vs axillary) found that nerve blocks were superior to hematoma block to provide pain control and decrease pain during manipulation of the fracture.

Reduction and Splinting
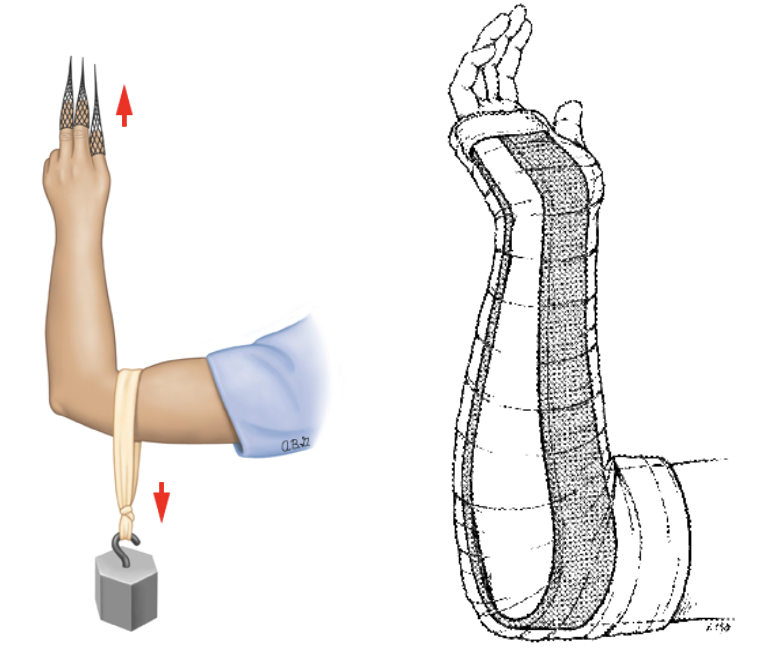
The technique used for fracture reduction will depend on the type of distal radius fracture. However, the main goal is to recreate and then reverse the mechanism of injury. Prior to reduction, finger traps are used to provide traction and hang the arm with the elbow 90-degree flexion and the forearm in neutral position. Weights are also placed on the distal humerus to provide counter-traction. This technique helps to relax the muscles prior to reduction.
The Sugar Tong:
After reduction, the most common splint used for distal radius fractures is the Sugar Tong splint. Just like with any other splint, neurovascular status must be assessed prior to applying the splint. All the material should be pre-measured prior to application, including the stockinette, Webril, and plaster. The plaster is applied from the palmar crease and is wrapped around the elbow, ending at the MCPs on the dorsum of the hand. Ace wrap is quickly applied and the material is molded to the desired shape. This position is held until the material hardens. YOU MUST re-check neurovascular status and then obtain post-reduction XR.
References
Boggess, B. R. (2023, June 5). Anatomy and basic biomechanics of the wrist. UpToDate. https://www.uptodate.com/contents/anatomy-and-basic-biomechanics-of-the-wrist?search=distal+radius+fracture&topicRef=219&source=see_link
Siebelt, M. , Hartholt, K. , van Winden, D. , Boot, F. , Papathanasiou, D. , Verdouw, B. , de Vries, M. , Mathijssen, N. & Kraan, G. (2019). Ultrasound-Guided Nerve Blocks as Analgesia for Nonoperative Management of Distal Radius Fractures–Two Consecutive Randomized Controlled Trials. Journal of Orthopaedic Trauma, 33 (4), e124-e130. doi: 10.1097/BOT.0000000000001388.
https://radiopaedia.org/articles/frykman-classification-of-distal-radial-fractures?lang=us
Corsino CB, Reeves RA, Sieg RN. Distal Radius Fractures. [Updated 2023 Aug 8]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK536916/
https://wikem.org/wiki/Distal_radius_fractures
Petron, D. J. (2024, November 24). Distal radius fractures in adults. UpToDate. https://www.uptodate.com/contents/distal-radius-fractures-in-adults?search=distal+radius+fracture&source=search_result&selectedTitle=1~61&usage_type=default&display_rank=1#H15