
What’s the Point… the E-Point?
Written by: Dr. Tina Jagtiani
Edited by: Dr. Joann Hsu
The case:
This is a 55 year old male with past medical history of HFrEF, ischemic cardiomyopathy s/p SQ ICD, CAD s/p CABG and PCI, pAF on Xarelto, CKD, HTN, HLD, T2DM presenting to the emergency department for worsening shortness of breath for three days with associated leg swelling and dry cough. Patient denies orthopnea, chest pain or palpitations. He states he is normally compliant with medications however recently ran out with no refills.
Vitals:
BP: 137/91 HR: 88 RR: 16 T: 36.8 C SpO2 92% placed on 3L NC with improvement to 95%
Pertinent Physical Exam
Respiratory: mild respiratory distress, still able to speak in full sentences, mild crackles at the bilateral bases
Extremities: +1 pitting edema to the bilateral lower extremities
Bedside echo showed:
Parasternal long axis view was obtained which shows grossly reduced ejection fraction (EF) and no pericardial or pleural effusions.
Parasternal short axis view obtained with no regional wall abnormalities and again noted is the grossly reduced ejection fraction.
Following cardiac ultrasound, the lungs were scanned and B lines were appreciated in all lung fields bilaterally. The below images were taken from one lung field on either side.
EPSS & Background
E-point septal separation (EPSS) is a simple echocardiographic measurement that can provide an estimation of left ventricular ejection fraction (LVEF) and systolic function. It is particularly useful in the emergency and critical care settings where comprehensive echos are not readily available but knowing a patient’s LVEF is relevant to their emergent workup and management.
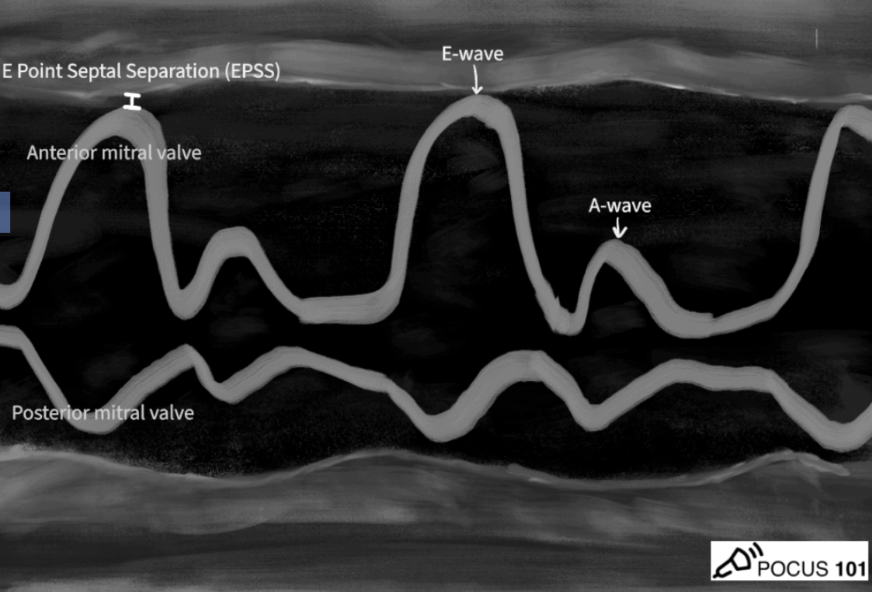
EPSS measures the distance between the fully open anterior mitral valve leaflet and the interventricular septum during early diastole.
The “E point” refers to the point of maximum early diastolic opening of the mitral valve and the “A point” refers to the atrial contraction later during left ventricular diastole.
The though process behind EPSS is that the opening of the mitral valve and how close the anterior mitral valve leaflet moves towards the interventricular septum = a surrogate for LVEF.
In a normal preserved LVEF, the anterior mitral valve leaflet hits the interventricular septum when fully open. EPSS measurement is essentially 0.
As the LVEF decreases, the mitral valve opens less and less, making the EPSS measurement (aka the distance between mitral valve and interventricular septum) greater.
Technique
Obtain parasternal long axis view using phased array (cardiac) probe
Activate M mode
Position the M mode line so it crosses the distal tip of the anterior mitral valve leaflet when it is at its most open, or when it gets closest to the interventrular septum.
Hit M mode again to obtain the tracing.
Freeze the image and measure the minimum distance from the E- point to the septum
Take the average over 3-5 cycles
Interpretation
Conventionally, 7 mm is the upper limit of normal for a preserved ejection fraction.
A normal ejection fraction is considered to be ≤ 7 mm and reduced ejection fraction is > 7 mm.
EPSS values ≥ 13 mm are severely reduced with an estimated left ventricular ejection fraction of < 35%.
Of note, there is still some discrepancy as to what cutoff threshold represents reduced ejection fraction based on the study you are referencing, so it is safe to say the extremes of the continuum are more widely accepted.
Visual estimation of ejection fraction on ultrasound has actually shown to be comparable to, and in some cases, even superior to calculating the EPSS.
Visual estimation by skilled sonographers can be performed faster and is particularly useful in an emergency setting with time constraints.
EPSS however, can assist in a more objective measurement / estimation of LVEF and can be used in conjunction with visual estimation.
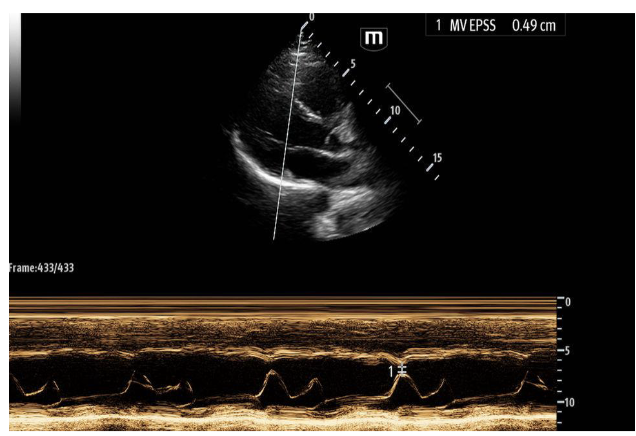
These echo images are examples of a heart with a normal ejection fraction. M mode was utilized to calculate an EPSS of 0.49 cm or 4.9 mm.
Advantages of EPSS
There are several advantages to utilizing EPSS in the emergency department, some of which are listed below:
Quick and easy to perform, even for less experienced sonographers
Quantitative measurement with limited subjectivity
Does not require complex calculations
Good for serial assessments
Limitations of EPSS
As with anything, there are several limitations to EPSS that one should be aware of when using it and interpreting the data. Some limitations are listed below:
Can be inaccurate (falsely elevated) in patients with history of hypertrophic cardiomyopathy, mitral stenosis or aortic regurgitation
Provides an estimate rather than precise measurement
Less specific than other methods to assess ejection fraction
Must be used in conjunction with visual estimation
Now back to the case, below is our patient’s recorded EPSS:
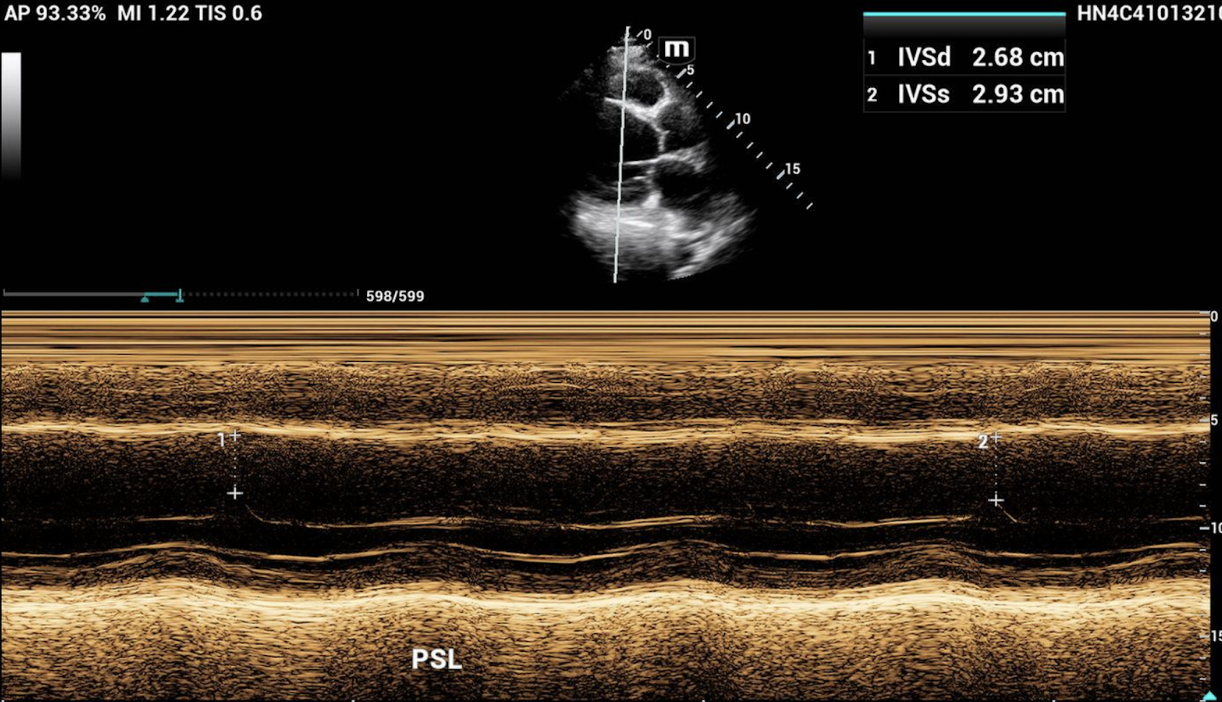
The EPSS was recorded at two separate intervals with an average of 2.81 cm or 28.1 mm, which is severely reduced.
The patient was admitted foracute hypoxic respiratory failure 2/2 acute on chronic CHF exacerbation
During admission, an official echocardiogram was done which showed a mildly dilated left atrium and left ventricle, left ventricular systolic function reduced with EF of 30-35% and moderate global hypokinesis of left ventricle.
Happy scanning!
References
5 MIN Sono – Basic cardiac function. (2024, June 4). Core Ultrasound - free and subscription ultrasound education for medical professionals. https://coreultrasound.com/basic-cardiac-function/
Advanced critical care ultrasound: E-point septal separation to estimate left ventricular ejection fraction. (2021, May 26). Your Home EMRA. https://www.emra.org/emresident/article/epss
Ahmadpour H, et al. The sensitivity and specificity of various echocardiographic indices in the diagnosis of impaired left ventricular function. Clin Cardiol. 1983;6(1):37-41.
Assessing left ventricular ejection fraction with echocardiography. (2024, November 7). POCUS 101. https://www.pocus101.com/assessing-left-ventricular-ejection-fraction-with-echocardiography/#E-Point_Septal_Separation_EPSS
Massie BM, et al. Relation of echocardiographic M-mode findings to severity of coronary artery disease and left ventricular dysfunction in aortic regurgitation. Am J Cardiol. 1977;40(6):903-910.
McKaigney CJ, et al. E-point septal separation: a bedside tool for emergency physician assessment of left ventricular ejection fraction. Am J Emerg Med. 2014;32(6):493-4974.