
Ketamine Compared With Morphine for Out-of-Hospital Analgesia for Patients With Traumatic Pain A Randomized Clinical Trial
Written By: Arrianna Mohammed, MD; Edited By: Brian Smith, DO, MA, MMsc-Med

What is the study question?
Is intravenous ketamine hydrochloride noninferior to intravenous morphine sulfate in adults with out-of-hospital traumatic pain?
What study design is used to answer the question?
The Intravenous Subdissociative-Dose Ketamine Versus Morphine for Prehospital Analgesia (KETAMORPH) study was a prospective, multicenter, single-blind, noninferiority randomized clinical trial to compare the effect of intravenous ketamine with that of intravenous morphine in the treatment of adults with out-of-hospital traumatic pain.
What is the exposure or intervention?
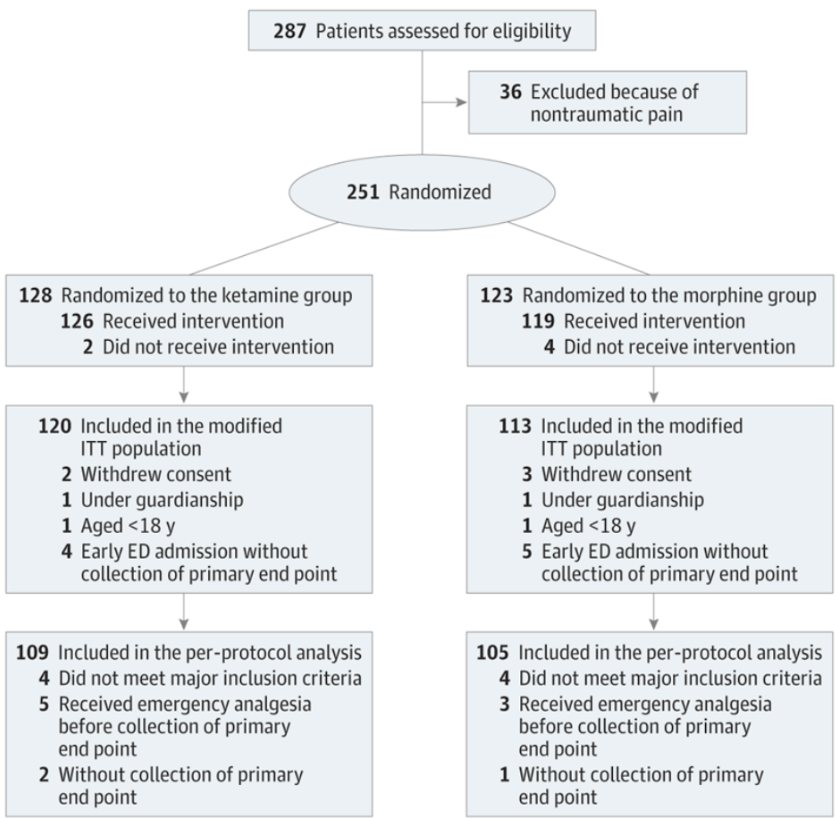
Patients were randomly assigned to ketamine (n = 128) or morphine (n = 123). Total 251 patients included in the study
IV push of Ketamine IV 20mg for 2 mins followed but IV push of 10mg every 5 mins (200mg total)
IV push of 2mg Morphine (weight <60mg) or 3mg (weight >60mg) every 5 mins (10mg total)
What is the outcome (or disease) and how is it measured (or defined)?
The primary outcome was the between-group difference in mean change in verbal rating scale pain scores measured from the time before administration of the study drug to 30 minutes later. A noninferiority margin of 1.3 was chosen.
How were participants selected or recruited for the study?
This study, performed between November 23, 2017, and November 26, 2022, involved 11 out-of-hospital emergency medical services (EMS) centers in France. These centers are ambulance base stations equipped with 1 or more mobile intensive care units consisting of an ambulance driver, a nurse, and an emergency physician as the minimum team.
Who was included in the study?
Aged 18 years or older
Conscious (Glasgow Coma Scale score of 15
Reporting acute traumatic pain with a verbal numeric rating scale pain score of 5 or greater on a standard 11-point numeric rating scale (where 0 indicates no pain and 10, worst possible pain), speaking, and being able to rate their pain with the verbal numeric rating scale.
Who was excluded from the study?
Unstable vital signs (systolic blood pressure <90 or >200 mm Hg, pulse rate <50 or >150 beats/min, and respiration rate <10 or >30 breaths/min)
Pregnancy, breast-feeding
Unable to rate their pain with the verbal numeric rating scale scores
Allergy to morphine or ketamine
Acute pulmonary edema or acute heart failure, acute coronary syndrome or unstable ischemic heart disease
Renal or hepatic insufficiency
Head injury with acute intracranial hypertension
Receiving buprenorphine hydrochloride, nalbuphine hydrochloride, pentazocine hydrochloride, or naltrexone hydrochloride
When did randomization occur?
Patients were randomized in a 1:1 ratio to the ketamine or the morphine group (Figure 1). A computerized random number generator created the randomization list (1:1). Central randomization was defined without block but was stratified by center. Group assignments were then sent in sealed envelopes to the study centers.
What do the authors say about power/sample size of the study? Is the power adequate to answer the study question?
After assuming a noninferiority margin of 1.3 with a type I error of 5%/2 and type II error of 10%, we determined that 224 patients were needed (112 in each treatment group). We set targeted enrollment at 248 patients to account for the risks of protocol deviations, considering that 10% of patients may not be evaluable.
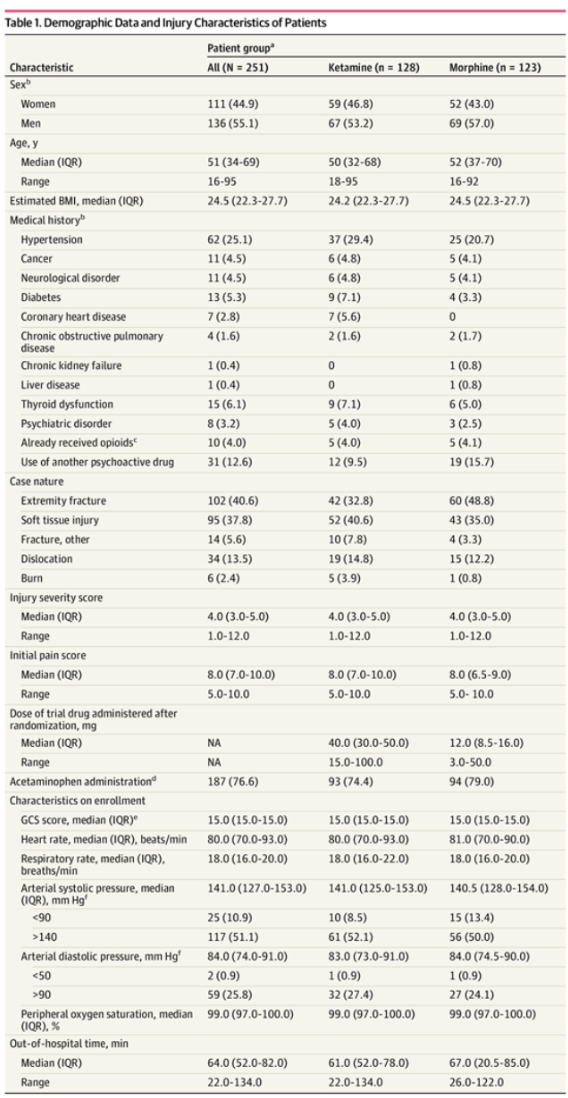
Are the study groups’ characteristics comparable at baseline?
Patient characteristics were well balanced between the 2 groups except for history of diabetes and coronary heart disease (Table 1). None of the observed differences appeared to be clinically meaningful.
What statistical tests/methods are used in the analysis of the results? Is the “intention to treat” principle maintained (if the study is a clinical trial)?
Intention to treat principle was not maintained. Followed a per-protocol analysis in selection.
What are the results of the study?
The mean pain score change was −3.7 (95% CI, −4.2 to −3.2) in the ketamine group compared with −3.8 (95% CI, −4.2 to −3.4) in the morphine group. The difference in mean pain score change was 0.1 (95% CI, −0.7 to 0.9) points.
There were no clinically meaningful differences for vital signs between the 2 groups. The intravenous morphine group had 19 of 113 (16.8% [95% CI, 10.4%-25.0%]) adverse effects reported (most commonly nausea [12 of 113 (10.6%)]) compared with 49 of 120 (40.8% [95% CI, 32.0%-49.6%]) in the ketamine group (most commonly emergence phenomenon [24 of 120 (20.0%)]). No adverse events required intervention.
Are the results statistically significant?
Yes, they are statistically significant.
Are the results clinically significant?
Yes, they support that ketamine may be a good option for certain populations to reduce opioid use for pain control.
What are the biases/limitations of the study that could cause you to question the author’s conclusions?
First, the presence of a physician in the ambulance team may make the results of this study less relevant for US-based EMS systems where the number and training of available out-of-hospital clinicians clearly differ.
Second, doses of morphine used in the trial were based on French recommendations, using small starting dose that may be less prone to provide rapid analgesia.
Third, the single-blind design could have introduced performance bias.
Fourth, we used a noninferiority design, but we were not able to show superiority in clinical secondary end points.
Fifth, the follow-up time was limited to the out-of-hospital period, which limits the conclusions of the study, as patients in the ketamine arm may have been exposed to opioids during their subsequent hospital care.
Point out which limitations or biases are unique to the study design (see below), and discuss how these potential problems are addressed by the authors.
Inadequate blinding of participants and investigators to exposure/treatment
“The participants were blinded to the study arm in which they were enrolled but the physicians conducting the out-of-hospital pain management were not blinded for the following reasons: (1) patients receiving ketamine were expected to exhibit obvious and easily identifiable effects, making the study arm allocation obvious to the clinician and negating the intent of masking; (2) the need to double-check drugs and doses according to standard operating procedures to ensure patient safety; and (3) the primary outcome was assessed by the patient using the verbal rating scale without any possible intervention of the physician in charge of the patient, contrary to earlier research where the verbal rating scale ratings were measured by the physicians who administered the analgesic.”
Comment on the overall internal validity of this article. Did the authors rule out chance, bias, and confounding as explanations for their findings?
No, pain scores were verbal and is subjective. One side was not blinded.
Comment on external validity or generalizability of this study. Would these results change your practice? How do these results fit into what we already know about this subject? (Understand that to achieve internal validity discussed above researchers often sacrifice external validity)
Not as generalizable in the US. Most trials are out of hospital not in the ED.
How does this fit our current knowledge? (refer to current practice, previous beliefs, and/or previous studies)
Further confirms that there is utility of ketamine in reducing opiod use in certain patient populations but there are a lot of confounding factors to consider especially in the ED setting.
Potential limitations/biases according to study design:
Cross-Sectional
No way to establish temporal relationship exposure and outcome measured at the same time.
Selection Bias
Self-Reporting Bias
Response Bias
Case-Control
Selection Bias (of cases and controls)
Recall Bias
Questionable Temporal Relationship (decrease exposure before outcome)
Cohort
Selection Bias
Loss to Follow up
Change in habits over time
Experimental Design
Selection Bias
Loss to Follow up
Improper or biased randomization procedures
Inadequate blinding of participants and investigators to exposure/treatment