
Anatomy of a Nightmare: Unstable C-Spine Fractures
Written By: Callie Winters, MD; Edited by: Timothy Khowong, MD, MSEd
Review of the Anatomy:
The cervical spine consists of 7 vertebrae. C1 is also referred to as the “atlas” and C2 is also referred to as the “axis”. The remainder of the cervical vertebrae (C3-C7) are referred to as “sub-axial”.


Common Etiologies and Epidemiology of C-Spine Fractures:
C1 fractures are often the result of axial loading. C2 are often a combination of compression and hyperextension or hyperflexion and account for approx. 30% of all c-spine fractures. Sub-axial fractures often result from high-impact trauma. C7 fractures account for another 20% of all c-spine fractures 1.
General Indications of an Unstable C-Spine Fracture:
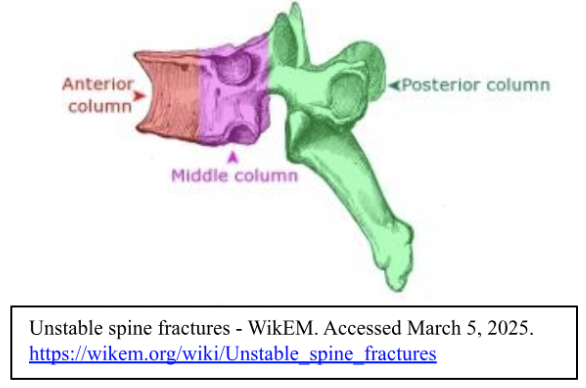
Fractures that result in an increase or decrease in intervertebral disc height, an increase in interspinous distance, involve facet joint widening, or involve significant vertebral compression (>25%) are all general indications for instability1. Denis’ three column concept separates the spine into the anterior, middle, and posterior column. Fractures that involve just the anterior column are most likely stable, fractures involving the middle column may be unstable, and fractures involving the posterior column are going to be unstable fractures. Fractures involving two or more columns are likely to be unstable 2.
There are a number of specific fracture types that are likely to be unstable, these include:
Jefferson Fractures
Bilateral facet dislocations
Odontoid type 2 and 3 fractures
Atlanto-occipital dislocation
Hangman’s fractures
Teardrop fractures
Jefferson Fractures:
This eponymous injury is a burst fracture of the atlas (C1). It’s mechanism is most likely to be axial load, such as in the case of a person diving head first into a shallow pool. This fracture is associated with vertebral artery injury, additional c-spine injuries, concurrent intracranial injury in young children, and in cranial nerve injuries. The instability of these fractures is due in large part to accompanying disruption of the transverse atlantal ligament, and when this ligament is disrupted aggressive management will be necessary with halo immobilization or internal fixation 3, 4.


Bilateral Facet Dislocations
In the young these injuries are usually associated with high-energy trauma, but they can result from low-energy trauma in the elderly. 17% of facet dislocations/fractures occur at the C7-T1 junction or are fractures of C7. The dislocation of the facets bilaterally and ligamentous disruption allows for severe subluxation of the spine (≥50%), and this in turn can result in 80% of these injuries being associated with spinal cord injury. Treatment of these injuries is surgical 5, 6.


Odontoid Fractures (Type I and II):
Odontoid fractures, or fractures of the dens of the axis (C2). Like in bilateral facet dislocation these are most common with high energy trauma in the young, but can be seen after low energy trauma in the elderly. Neck pain with movement, especially rotation, can be present. These fractures are associated with hyperflexion or hyperextension. Type II and III odontoid fractures are unstable. Type II fractures have a high risk of nonunion. Treatment may be collaring, halo vest, or surgical intervention depending on risk of nonunion, patient age, and other factors. Outcomes in patients >80 years of age are poor regardless of intervention 7.

Atlanto-Occipital Dislocation:
Involves disruption of the ligaments at the articulation of the atlas (C1) and the occipital bone. Colloquially referred to as “internal decapitation”, this condition is often, though not exclusively, rapidly fatal. Treatment is usually internal fixation, though many of these patients will have experienced cardiopulmonary arrest prior to arrival at the hospital 8, 9.

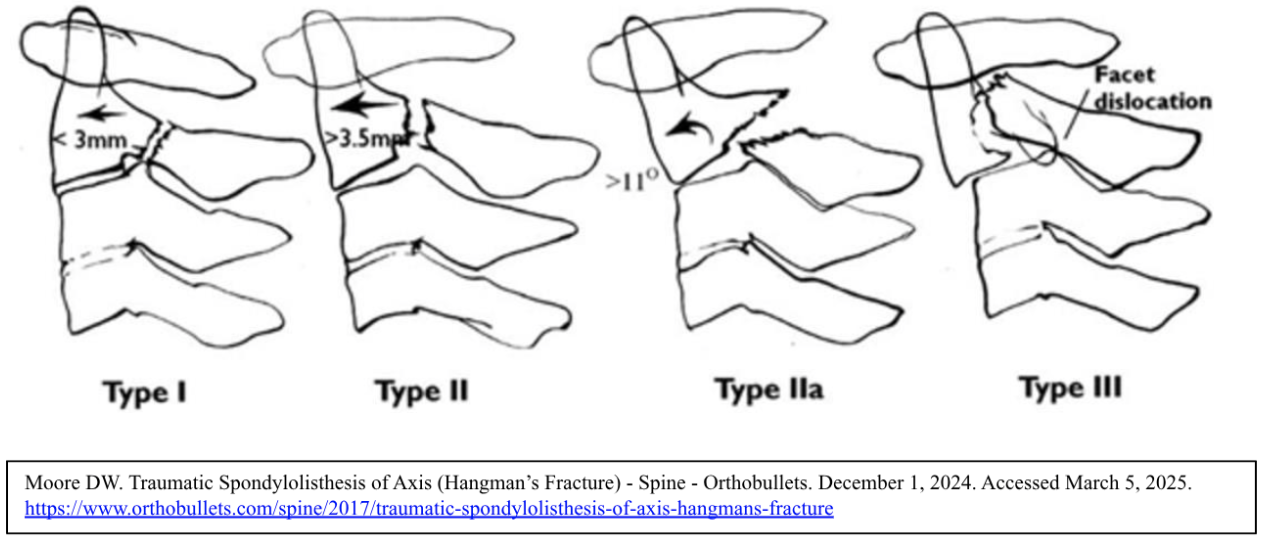
Hangman’s Fracture:
This refers to a bilateral fracture of the pars interarticularis of the axis (C2), it is also referred to as traumatic spondylolisthesis of the axis. It is associated with hyperextension followed by secondary flexion, which allows for subluxation. These fractures also have a grading system, and Type I fractures may be non-operative, however higher grade fractures will require halo immobilization and/or surgical fixation.
Flexion Teardrop Fracture
These are injuries of severe flexion/compression that are associated with significant ligamentous disruption and instability. They are associated with spinal cord injury including quadriplegia and anterior cord syndrome. The injury pattern is most associated with spinal levels C4, C5, C6. Most patients will require decompression and internal fixation. Of note, extension teardrop injuries are also possible, but are usually found at higher spinal levels and are considered less severe 11.

Evaluation and Management of Unstable C-Spine Fractures in the Emergency Department:
Immobilization with a properly sized and placed c-collar is of paramount importance. Extreme care should be taken when moving the patient. Initial evaluation should include a complete and thorough neurological exam- depending on the level of the injury the patient’s respiratory status may be compromised or become compromised over time. On the other hand, not all unstable c-spine fractures will present with neurological deficits- even significant injuries that will lead to high morbidity or mortality over time may present with deceptively unremarkable physical exam findings and mild reported symptoms, so suspicion should remain high and the threshold to pursue imaging should remain low especially in the elderly. CT is the initial imaging modality of choice, though follow up MRIs may be required to assess cord and ligamentous injury 2. Consultation with neurosurgery, orthopedic surgery, and/or trauma surgery may be indicated.
Sources:
1 Gaillard F, Mellam Y, Bell D, et al. Cervical spine fractures. Reference article,
Radiopaedia.org (Accessed on 06 Mar 2025) https://doi.org/10.53347/rID-1089
2 Unstable spine fractures - WikEM. Accessed March 5, 2025.
https://wikem.org/wiki/Unstable_spine_fractures
3 Agrawal R, Knipe H, Deng F, et al. Jefferson fracture. Reference article, Radiopaedia.org
(Accessed on 06 Mar 2025) https://doi.org/10.53347/rID-1534
4 Wong A, Knipe H, Bell D, et al. Cruciate ligament of the atlas. Reference article,
Radiopaedia.org (Accessed on 06 Mar 2025) https://doi.org/10.53347/rID-36585
5 Forsthoefel C, Moore DW. Cervical Facet Dislocations & Fractures - Spine - Orthobullets.
Orthobullets. June 7, 2021. Accessed March 5, 2025. https://www.orthobullets.com/spine/2064/cervical-facet-dislocations-and-fractures
6 Goel A, Feger J, Spires R, et al. Bilateral facet dislocation. Reference article,
Radiopaedia.org (Accessed on 06 Mar 2025) https://doi.org/10.53347/rID-35385
7 Moore DW. Odontoid Fracture - Spine - Orthobullets. November 30, 2024. Accessed
March 5, 2025. https://www.orthobullets.com/spine/2016/odontoid-fracture
8 Joaquim AF, Schroeder GD, Vaccaro AR. Traumatic Atlanto-Occipital Dislocation—A
Comprehensive Analysis of All Case Series Found in the Spinal Trauma Literature.
Int J Spine Surg. 2021;15(4):724. doi:10.14444/8095
9 Asfaw T, Chow B, Frederiksen RA. Atlanto-occipital dislocation: Case report and
discussion. Radiology Case Reports. 2011;6(4):573. doi:10.2484/rcr.v6i4.573
10 Moore DW. Traumatic Spondylolisthesis of Axis (Hangman’s Fracture) - Spine –
Orthobullets. December 1, 2024. Accessed March 5, 2025.
https://www.orthobullets.com/spine/2017/traumatic-spondylolisthesis-of-axis-
hangmans-fracture
11 Harvey H, Elfeky M, Yap J, et al. Flexion teardrop fracture. Reference article,
Radiopaedia.org (Accessed on 06 Mar 2025) https://doi.org/10.53347/rID-15003