
Spilling the Teacup: Lunate and Perilunate Dislocations
Written by: Boyd Qu, MD; Edited by: Timothy Khowong, MSEd
Case:
First, let’s start with a case. An elderly 71 year old female comes in after a mechanical trip and fall with left wrist pain while walking on pavement. The patient says that she landed with an outstretched hand. An X-ray is obtained and is shown below:
What is the diagnosis? What should the immediate next steps be?

Today, we’ll be talking about lunate and perilunate dislocations and fractures! These are a relatively rare injury and they make up approximately 7% of all injuries to the wrist bones. [1]
Anatomy:

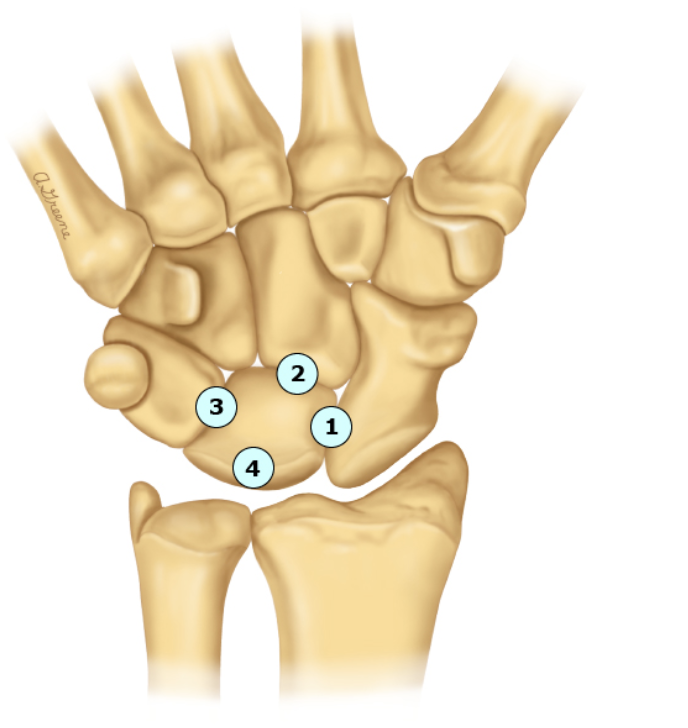
The lunate is a crescent-moon shaped (makes sense why it’s called the lunate bone) carpal bone that sits in the proximal row. It’s attached to its carpal bones by interosseous ligaments and is further stabilized by ligaments connecting it to the radius, ulna and distal carpal bones. The bone itself receives dual blood supply from branches of both the radial and ulnar arteries. Interestingly enough, 20% of individuals only receive blood supply for the lunate bone from one artery! These individuals are at particularly high risk of suffering from avascular necrosis after a lunate injury.
Mechanism of Injury:
Lunate and perilunate dislocations and fractures most frequently occur after a FOOSH. As more and more force is applied to this bone, there’s a predictable sequence of injuries that will occur as follows:
The scapholunate ligament ruptures which causes instability between the scaphoid and lunate.
The capitolunate ligament will rupture causing dislocation of the capitate (not always).
Lunotriquetral ligament ruptures and the lunate dislocates dorsally.
The lunate dislocates in the volar direction.
Physical Exam:

Here, you can see the lunate bone marked with the “L”. The lunate bone is directly in line with the 3rd metacarpal bone. Physical exam will usually reveal tenderness in the dorsal aspect of the middle of the wrist made worse by movement or squeezing the fingers together. If a dislocation is present, there may be a fullness either dorsally or vorsally depending on the direction of displacement.
An assessment of the nerves of the hand is critically important as any sort of nerve injury is an orthopedic emergency! If the lunate dislocates volarly into the carpal tunnel, it may impinge on the median nerve. This is associated with decreased sensation in the thumb, index, and middle fingers and radial half of the ring finger. There may also be decreased strength in the thumb and grip strength.
Imaging:
X-rays are first line in the setting of a patient suffering from wrist pain and trauma. Here, below you can see on the left a normal wrist X-ray and on the right a perilunate dislocation.

The lunate on the right is anterior and distally displaced, almost like a spilled tea-cup!
These injuries are obvious and rarely missed on X-ray, but subtle fractures of the lunate bone are often missed. CT and MRI are the gold standard. Some studies have shown that X-rays can have sensitivities as low as 20%. Yikes!
For scapholunate dissociations, a widening of the space >3mm is suggestive of a scapholunate dissociation (below).

Treatment:
When a dislocation is present, immediate orthopedic consultation and reduction should be performed. When there’s compromise of the median nerve, reduction is paramount to preserving hand strength and function.
The general technique involves the “finger-trap” method where the patient’s fingers are hung from an IV pole via some gauze. Traction is applied at the elbow, with the elbow flexed at 90 degrees (left).
After 15 minutes of traction has been applied, the wrist is extended first. Then, traction is applied with your thumb pushing the lunate bone back into place while flexing the wrist (middle).
Afterwards, a sugar tong splint should be applied. Patients need to followup within 72 hours at a hand clinic. Some experts argue that operative reduction and fixation has better outcomes, but this is still not the standard of care currently (right).



References:
Sawardeker PJ, Baratz ME. Carpal injuries. In: DeLee & Drez’s Orthopaedic Sports Medicine: Principles and Practice, 4th ed, Miller MD, Thompson SR (Eds), Saunders Elsevier, Philadelphia 2015.
https://radiopaedia.org/cases/normal-lateral-wrist-radiograph
Welling RD, Jacobson JA, Jamadar DA, Chong S, Caoili EM, Jebson PJ. MDCT and radiography of wrist fractures: radiographic sensitivity and fracture patterns. AJR Am J Roentgenol. 2008 Jan;190(1):10-6. doi: 10.2214/AJR.07.2699. PMID: 18094287.
https://www.orthobullets.com/hand/6045/lunate-dislocation-perilunate-dissociation