
Pain and Strain
Brian Smith, DO
You are working a busy shift in the ED when the tech hands you this ECG:
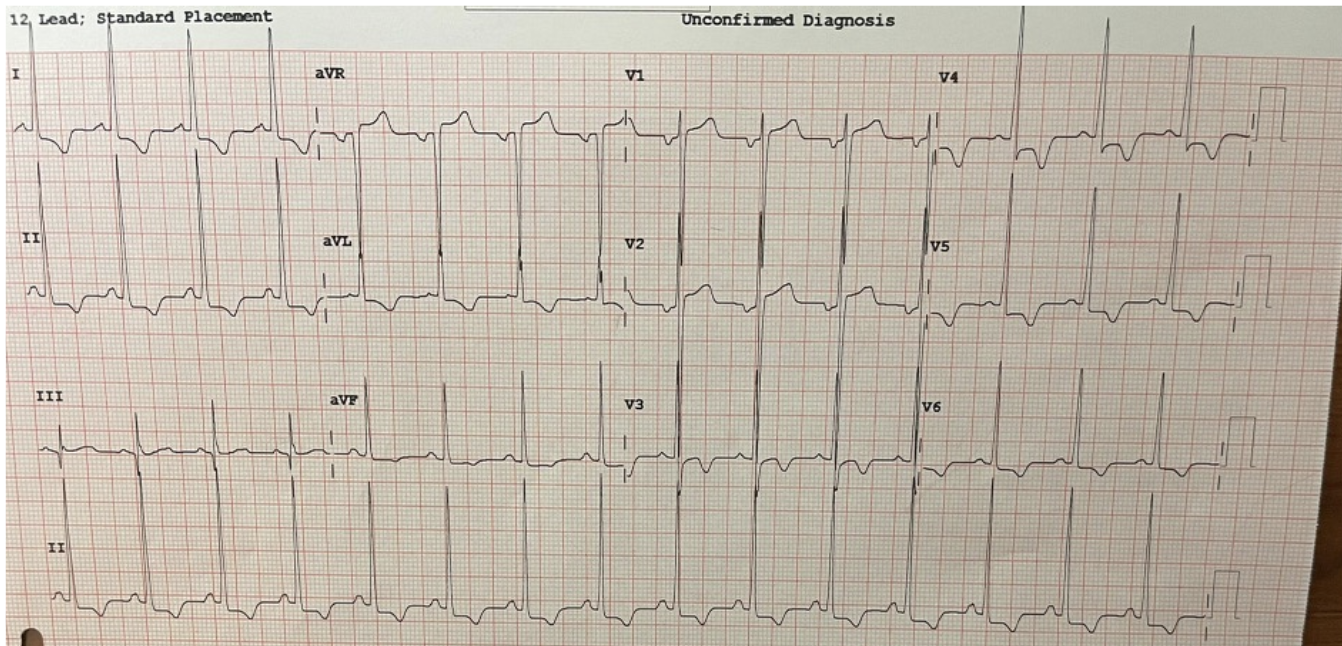
The tech informs you the patient is presenting with epigastric pain and vomiting. She says the patient looks uncomfortable. You do a quick chart review and find this patient is a 74 M with a PMH HTN, HLD, DM presenting with epigastric pain and vomiting x 4 hours.
VS: BP 190/85, HR: 90, RR: 18, Temp: 36.8 oral, Weight: 85 kg, FS: 180
You have no prior ECG for comparison.
What do you want to do for this patient?
A) This ECG is concerning for STEMI, activate cath lab
B) See patient immediately and obtain repeat ECG
C) Send to the main emergency department with telemetry monitoring
D) Sent the patient to the waiting room
Think about your answer before scrolling down! What pattern does this ECG represent?
LEFT VENTRICULAR HYPERTROPHY:
This ECG is suggestive of Left Ventricular Hypertrophy (LVH), likely secondary to chronic remodeling from longstanding hypertension. This is NOT a STEMI or STEMI equivalent
There are many different voltage criteria used to detect LVH. Life in the Fast Lane uses the following:
Limb Leads:
R wave in lead 1 + S wave in lead iii > 25 mm
R wave in aVL > 11 mm
R wave in aVF > 20 mm
S wave in aVR > 14 mm
Precordial Leads:
R wave in V4, V5, or V6 > 26 mm
R wave in V5 or V6 + S wave in V1 > 35 mm
Largest R wave + Largest S wave > 45 mm
This seems like A LOT to remember. There has to be a better way to cognitively offload and rapidly assess for LVH on ECG…..right?
Seamens’ Sign:
Well, in May 2022, Walker et. al. published a paper titled “Seamens' Sign: a novel electrocardiogram prediction tool for left ventricular hypertrophy” that asked the same question.
In this study, the authors performed a retrospective chart review to see if a simplified voltage criteria dubbed “Seamen’s Sign” stood up to the many other voltage criteria for LVH.
What is Semen’s Sign? QRS complexes touching or overlapping in 2 contiguous precordial leads.
Simple right? But how does it measure up to other voltage criteria?
Seamen’s sign was found to be 92% specific for LVH AND was noninferior to all other voltage criteria other than Cornell Criterion for Women

Again, here on our patient’s ECG, we see overlapping QRS complexes in 3 contiguous leads. (blue circles). This is positive Seamen’s Sign, suggestive of LVH
But What About the ST Depressions in the Lateral LEads?
Concerning, right? I see residents often confusing this for acute ischemia, but these ST depressions are representative of LVH WITH STRAIN
WHAT IS STRAIN?
SInce patients with LVH have a thickened LV wall, they will have PROLONGED DEPOLARIZATION and DELAYED REPOLARIZATION.
Signs of both can be seen on ECG:
Prolonged Depolarization: Increased R wave peak time > 50 ms in V5 or V6
Delayed Depolarization: ST depressions and T wave inversions in lateral leads - This is known as strain pattern

“Strain pattern”: ST depressions in the lateral leads. (red boxes)
Back To OUr Patient:
The patient was seen immediately by providers. He was laying in the stretcher, writing in pain and actively vomiting. Heart and lungs are clear. His abdominal is mildly distended and minimally tender throughout.
Repeat ECG is performed and unchanged from prior
A bedside ultrasound was attempted, but patient was unable to tolerate it due to pain
Labs, imaging, fluids, pain meds, antiemetics were ordered. Given the patient’s pain out of proportion to exam, a CTA abd/pelvis was ordered to evaluate for mesenteric ischemic.
On POC blood testing: Lactate was 9 and patient is hypokalemic to 2.7, otherwise labs was wnl
CT found CLOSED LOOP SBO. patient given pain meds, IV fluids, K+ repletion, NG tube was placed, and patient was admitted to surgical service and went straight to OR
He eventually recovered and was discharged home
Take Home Points
There are many voltage criteria for LVH, but look for Seamens’ Sign as a quick and easy way to assess for LVH on ECG
ST depressions in lateral leads in the setting of LVH are suggestive of Strain Pattern, and are often confused for acute ischemia
If you are concerned about a patient’s ECG, look for a prior and obtain a repeat to assess for dynamic changes
Thanks for playing!
〰️
Thanks for playing! 〰️
References:
Burns, Ed, et al. “Left Ventricular Hypertrophy (LVH).” Life in the Fast Lane • LITFL, 1 Apr. 2021, https://litfl.com/left-ventricular-hypertrophy-lvh-ecg-library/.
Walker P;Jenkins CA;Hatcher J;Freeman C;Srica N;Rosell B;Hanna E;March C;Seamens C;Storrow A;McCoin N; “Seamens' Sign: A Novel Electrocardiogram Prediction Tool for Left Ventricular Hypertrophy.” PeerJ, U.S. National Library of Medicine, https://pubmed.ncbi.nlm.nih.gov/35669958/.